Yes, high cortisol levels, often associated with chronic stress, can negatively impact eyesight and contribute to various vision problems.
Cortisol, the body's primary stress hormone, can disrupt blood flow to the eyes and brain, potentially leading to issues like blurry vision, eye strain, increased light sensitivity, and in severe cases, even contribute to conditions like glaucoma.
Increased Eye Pressure: Elevated cortisol levels have been associated with an increase in intraocular pressure. Over time, this can lead to a greater risk of developing glaucoma, a potentially sight-threatening condition.
Dry Eyes: Stress can contribute to the development or exacerbation of dry eye syndrome.
Stress hormones include, but are not limited to, cortisol, catecholamines such as adrenaline and norepinephrine, vasopressin, and growth hormone.
Stress hormones play a complex role in fighting diseases and infections, as they can have both positive and negative effects on the immune system.
Here's a more detailed explanation:
Cortisol's Role:
Cortisol is released in response to stress, triggering a "fight-or-flight" response that can affect various bodily functions, including those of the eyes.
Impact on Blood Flow:
High cortisol levels can disrupt blood flow from the eye to the brain, potentially causing vision problems.
Stress-Related Vision Problems:
Blurry Vision: Stress can cause muscles around the eyes to tense up, leading to temporary or persistent blurry vision.
Chronic stress and elevated cortisol levels can manifest in several ways, including:
Eye Strain: Muscle tension and focusing difficulties due to stress can cause eye strain.
Increased Light Sensitivity: Some individuals may experience heightened sensitivity to light under stress.
Eye Twitching: Muscle spasms in the eyelids, often triggered by stress, can lead to eye twitching.
Headaches: Stress-related headaches can also impact vision.
Long-Term Effects:
Chronic stress and high cortisol levels may contribute to more serious eye conditions over time, such as glaucoma and optic nerve damage.
Managing Stress for Eye Health: Managing stress through techniques like relaxation exercises, mindfulness, and regular eye exams can help mitigate the negative impact of cortisol on vision.
Seeking Professional Help: If you experience persistent vision problems, especially if they coincide with stress or other health issues, it's crucial to consult with an eye care professional for proper diagnosis and management.
Normal cortisol levels vary throughout the day, typically peaking in the morning (around 6-8 AM) and reaching their lowest point at night (around midnight). For a blood test, the normal range in the morning (6-8 AM) is generally 10-20 micrograms per deciliter (mcg/dL) or 275-555 nanomoles per litre (nmol/L), while around 4 PM, it's usually 3-10 mcg/dL or 80-275 nmol/L. These ranges can vary slightly between laboratories.
More Details:
Diurnal Rhythm: Cortisol follows a circadian rhythm, meaning its levels fluctuate naturally throughout the day.
Morning Peak: Cortisol levels are typically highest in the morning, helping to prepare the body for the day's activities.
Afternoon Decline: Cortisol levels gradually decrease throughout the day, reaching their lowest point at night.
Lab Variation: Normal ranges can differ slightly between laboratories due to differences in testing methods and reference ranges.
Other Factors: Factors like age, health conditions, medications, and stress levels can also influence cortisol levels.
Anxiety and stress are two different terms that are often confused.
Stress is a process in response to environmental demands. It would be the physiological response of our organism. In this process, we interpret whether or not we are going to be able to give an adaptive response. If this is not the case, we perceive a threat that triggers the emotional response, which is what we call Anxiety.
Intense and sustained stress causes a series of hormonal alterations in the body, such as hypersecretion of cortisol and increased secretion of prolactin and melatonin, which inhibit ovulation and interfere with reproduction, making it difficult to achieve pregnancy in a natural way. The effect of cortisol in the body is to maintain vital signs and block those functions that are not necessary for survival.
In addition to cortisol, the brain also sends signals to manufacture adrenaline in response to fight or flight. This hormone causes an increase in blood pressure and heart rate.
Retinoschisis is a condition that happens when your retina divides into two or more layers. Schisis means a split or a cleft. Retinoschisis affects the light-sensing layer of your retina and the layer of cells that transmits signals to your brain through the optic nerve.
This division of the layers can affect how well you see. Splits can occur in the center of the retina but are more likely at the periphery (outer edges).
What are the signs and symptoms of retinoschisis?
You may have no symptoms of the disease. If you do, symptoms that may happen with juvenile X-linked retinoschisis include:
Eyes that turn toward your nose (crossed eyes).
Eyes that move uncontrollably from one side to the other (nystagmus).
Loss of central (foveal) vision or side (peripheral) depending on where the split occurs.
Having farsightedness.
If you’ve developed acquired retinoschisis, you might find that you can’t see clearly on either side (loss of peripheral vision). You may not have any symptoms at all.
If you have retinoschisis and it becomes severe, or you also have retinal detachment, you may notice:
Floaters and flashers.
Distorted images.
Loss of central (foveal) vision or side (peripheral) depending on where the split occurs.
Are X-linked disorders male or female?
X-linked recessive diseases most often occur in males. Males have only one X chromosome. A single recessive gene on that X chromosome will cause the disease. The Y chromosome is the other half of the XY gene pair in the male.
Patterns of inheritance
Patterns of X-linked recessive inheritance in a royal family
In humans, inheritance of X-linked recessive traits follows a unique pattern made up of three points.
The first is that affected fathers cannot pass X-linked recessive traits to their sons because fathers give Y chromosomes to their sons. This means that males affected by an X-linked recessive disorder inherited the responsible X chromosome from their mothers.
Second, X-linked recessive traits are more commonly expressed in males than females.This is due to the fact that males possess only a single X chromosome, and therefore require only one mutated X in order to be affected. Women possess two X chromosomes, and thus must receive two of the mutated recessive X chromosomes (one from each parent). A popular example showing this pattern of inheritance is that of the descendants of Queen Victoria and the blood disease hemophilia.
The last pattern seen is that X-linked recessive traits tend to skip generations, meaning that an affected grandfather will not have an affected son, but could have an affected grandson through his daughter. Explained further, all daughters of an affected man will obtain his mutated X, and will then be either carriers or affected themselves depending on the mother. The resulting sons will either have a 50% chance of being affected (mother is carrier), or 100% chance (mother is affected). It is because of these percentages that we see males more commonly affected than females.
X-Linked Retinoschisis (XLRS)
A rare disorder involving multiple structure of the eye characterized by reduced visual acuity in males due to juvenile macular degeneration. Clinical features such as vitreous hemorrhage, retinal detachment, and neovascular glaucoma can be observed in advanced stages.
X-linked Retinoschisis or X-Linked Juvenile Retinoschisis is a rare congenital disease of the retina caused by mutations in the RS1 gene, which encodes retinoschisis, a protein involved in intercellular adhesion and likely retinal cellular organization.
X-linked retinoschisis, with a prevalence of about 1 in 15,000 to 30,000, is one of the main causes of juvenile macular degeneration in males. It is characterized by symmetric bilateral macular involvement beginning in the first decade of life.
X-linked recessive genetic defects
It is caused by a large variety of mutations in theRS1 gene on Xp22.1-p22.3, which encodes the protein retinoschisis. This protein is involved in intercellular adhesion and likely retinal cellular organization. X-linked retinoschisis is inherited in an X-linked manner with complete penetrance and variable expressivity.
Most affected individuals are males, as heterozygous females are rarely affected. However, retinoschisis has been reported in non-consanguinous females. The phenotype can be markedly variable even within the same genotype and can involve the peripheral retina.
Preeclampsia and eclampsia are complications of pregnancy. The nurse plays a vital role in helping detect these conditions. Therefore, it’s important to know how to detect this condition in a pregnant patient.
The hormonal changes associated with pregnancy can impact a variety of things, including vision. In some cases, pregnant women may experience blurred vision as a result of high blood pressure. If vision loss is significant, this could be a sign of a serious health issue called preeclampsia. Typically occurring late in pregnancy, this condition can put both mother and child at serious risk if not treated. If you are pregnant and experiencing any significant vision problems, consult with your doctor immediately.
Blurred vision is the most common visual complaint. Focal or generalized arteriolar narrowing is the most common ocular finding in preeclampsia/eclampsia syndrome. Other ocular manifestations include photopsia, visual field defects, sudden inability to focus, and in severe cases, complete blindness.
Causes of Blurred or Distorted Vision
The preeclampsia/eclampsia syndrome is a multisystem disorder that can include cardiovascular changes, hematologic abnormalities, hepatic and renal impairment, and neurologic or cerebral manifestations. It also can affect the eye and visual pathways. Visual symptoms concern up to 25% of patients with severe preeclampsia and 50% of patients with eclampsia. This review discusses the ophthalmic complications of preeclampsia/eclampsia with focus on the hypertensive retinopathy, exudative retinal detachment and cortical blindness.
How common is preeclampsia?
Preeclampsia is a condition unique to pregnancy that complicates between 5% and 8% of all births in the United States. It’s also the cause of about 15% of premature deliveries (delivery before 37 weeks of pregnancy) in the U.S.
Preeclampsia is a serious medical condition that can occur about midway through pregnancy (after 20 weeks). People with preeclampsia experience high blood pressure, protein in their pee, swelling, headaches and blurred vision. But you may have no symptoms.
Treatment is necessary to avoid life-threatening complications. It typically goes away after childbirth.
Preeclampsia is a serious blood pressure condition that develops during pregnancy. People with preeclampsia often have high blood pressure (hypertension) and high levels of protein in their urine (proteinuria). Preeclampsia usually develops after the 20th week of pregnancy.
Preeclampsia can also affect other organs in your body and cause kidney and liver damage, brain injury and other serious side effects. It’s dangerous for both you and the developing fetus. Because of these risks, your healthcare provider will need to monitor your pregnancy closely and recommend treatment right away.
Preeclampsia Vision Changes
Preeclampsia is a hypertensive disorder affecting pregnant women, typically occurring after the 20th week of gestation.
In modern days, preeclampsia remains a leading cause of maternal and perinatal morbidity and mortality worldwide.
The most common symptoms include high blood pressure (hypertension) normally occurring in conjunction with proteinuria (presence of protein in the urine), signs of organ dysfunction, and preeclampsia vision changes.
The extended list of symptoms to look out for includes:
High blood pressure
Vision changes and disturbances
Proteinuria (presence of protein in the urine)
Excessive face & body swelling (edema)
Persistent and severe headaches
Pain or tenderness in the upper right side of the abdomen, just below the ribs
Pain or tenderness in the shoulder
Reduction in urine output (kidney dysfunction)
Severe nausea and vomiting in the second half of pregnancy
Shortness of breath
Another one of the prominent symptoms of preeclampsia is visual disturbances. They often occur during pregnancy and may persist postpartum.
The rise in blood pressure occurring with the condition affects organ systems, including the eyes. Which contributes to a range of visual difficulties. The fluctuations in vision can be alarming and significantly impact a woman's daily life, adding to the already substantial burden of this condition.
Preeclampsia vision changes commonly include blurry vision, light sensitivity (photophobia), and visual disturbances like seeingflashing lightsor floaters.
Preeclampsia vision changes may indicate potential severe complications.
Eye problems are way easier to detect than high blood pressure. So they are quite often the reason a pregnant woman or new mom gets the diagnosis and receives timely medical care.
Blurry vision
The vascular changes and low blood flow to the eyes affect visual function. Blurry vision may occur as a result of changes in the cornea, lens, or retina, leading to a decrease in visual acuity and sharpness. Fluid retention and eye swelling may contribute to blurriness.
Photophobia
Photophobia, as a preeclampsia symptom, makes individuals highly sensitive to light. Thus causing discomfort and a strong aversion to bright light sources. It can further lead to eye strain, headaches, and visual disturbances, adding to the burden of preeclampsia vision changes.
Preeclampsia Flashes
Flashes of light are another ocular discomfort we commonly associate with preeclampsia vision changes. These flashes, often described as brief, bright flickers or streaks of light, can appear suddenly and sporadically in a woman's visual field. Their occurrence is a result of abnormal retinal stimulation, due to vascular alterations.
Preeclampsia Floaters
Preeclampsia floaters are dark spots or specks that appear to "float" in a person's visual field. The causes are tiny protein or cell aggregations in the vitreous humor (the gel-like substance that fills the eye). They may appear as small dots or cobweb-like shapes, often moving with eye movements. Preeclampsia floaters are indicative of abnormal blood flow in the retinal blood vessels.
Flickers are sparkles that shimmer in vision("scintillations") Flickers usually come from activated visual cortex in migraine, but importantly also in transient ischemic attack, seizure, damaged retina, and damaged optic nerve.
Flashes are bright sparks or streaks of light that appear suddenly and briefly in vision
Flashes usually come from tugging on retinal photoreceptors, which may signal impending or actual vitreous detachment, retinal hole, or retinal detachment
Flickers are sparkles that shimmer in vision ("scintillations")
Flickers usually come from activated visual cortex in migraine, but importantly also in transient ischemic attack, seizure, damaged retina, and damaged optic nerveOcular migraines vs. migraine auras
Flashes appear abruptly like lightning bolts in outer edge of visual field
Flashes may be provoked by eye movement
Flickers may be transient or persistent
Flickers that are part of visual aura of migraine often expand across hemifield in 20-30 minutes and disappear
Flickers of migraine usually precede headache and other manifestations
Flickers of damaged retina or optic nerve are often persistent
In visual perception, flicker is a human-visible change in luminance of an illuminated surface or light source which can be due to fluctuations of the light source itself, or due to external causes such as due to rapid fluctuations in the voltage of the power supply (power-line flicker) or incompatibility with an external dimmer. eResearch by Navid Ajamin -- summer 2024
What is a migraine?
Migraine is a neurological condition that is characterized by often incapacitating symptoms including severe, throbbing and recurring pain that’s usually centered on one side of the head.
Other disabling symptoms of a migraine are nausea, vomiting, dizziness, tingling or numbness in the extremities or face, and extreme sensitivity to sound, light, touch and smell.
Migraine affects about 1 billion men, women and children worldwide and approximately 40 million Americans.
Migraine headaches can last up to three days and produce moderate to severe pain.
Migraines are most common between the ages of 18 and 44, and they affect women disproportionately. Eighteen percent of American women suffer from migraines, compared to 6 percent of men and 10 percent of school-age children.
There is a strong genetic link for migraines, with about 90 percent of sufferers reporting a family history of these headaches.
Migraine is a "diagnosis of exclusion," which means it is reached by a process of elimination since there is no test or biomarker to confirm its presence.
Just as every person is unique, so are migraine headaches. Migraines differ from person to person, and migraines also can present in different ways and with different symptoms in the same person.
Retinal migraine is a retinal disease often accompanied by migraine headache and typically affects only one eye. It is caused by ischaemia or vascular spasm in or behind the affected eye.
The terms "retinal migraine" and "ocular migraine" are often confused with "visual migraine", which is a far-more-common symptom of vision loss, resulting from the aura phase of migraine with aura. The aura phase of migraine can occur with or without a headache. Ocular or retinal migraines happen in the eye, so only affect the vision in that eye, while visual migraines occur in the brain, so affect the vision in both eyes together. Visual migraines result from cortical spreading depression and are also commonly termed scintillating scotoma.
Northern lights, aurora, borealis, scenic
Migraine aura
A migraine aura starts in your brain, not your eye. The aura is one or more symptoms that can happen right before a headache starts. These visual symptoms happen in both eyes.
Migraine with aura (also called classic migraine) is a recurring headache that strikes after or at the same time as sensory disturbances called aura. These disturbances can include flashes of light, blind spots, and other vision changes or tingling in your hand or face.
Treatments for migraine with aura and migraine without aura (also called common migraine) are usually the same. You can try to prevent migraine with aura with the same medications and self-care measures used to prevent migraine.
Symptoms
Migraine aura symptoms include temporary visual or other disturbances that usually strike before other migraine symptoms — such as intense head pain, nausea, and sensitivity to light and sound.
Migraine aura usually occurs within an hour before head pain begins and generally lasts less than 60 minutes. Sometimes migraine aura occurs without headache, especially in people age 50 and older.
Visual signs and symptoms
Most people who have migraine with aura develop temporary visual signs and symptoms, which tend to start in the center of the field of vision and spread outward. These might include:
Blind spots (scotomas), which are sometimes outlined by simple geometric designs
Zigzag lines that gradually float across your field of vision
Shimmering spots or stars
Changes in vision or vision loss
Flashes of light
Some people experience an aura without any pain at all. Doctors call this an “acephalgic migraine” or a “migraine aura without headache.”
It's also common for people to call them "visual migraines." This may be why they get mixed up with ocular migraines so often. Here is an easy way to remember the difference: "visual migraines" happen in your vision, but "ocular migraines" happen in your eye.
About 8% of the population gets migraines with aura.
One in every four people who get migraines sees an aura beforehand. Others will only experience symptoms like headache, nausea and vomiting.
Refer patient with flashes urgently to ophthalmologist because they suggest intraocular disorder (vitreous, retina, optic nerve)
Refer patient with flickers urgently to ophthalmologist, neuro-ophthalmologist or neurologist unless diagnosis of migraine is obvious because they could also suggest transient ischemic attack or seizure
Vitreous detachment may rarely cause retinal tear and detachment which must be repaired promptly to protect vision
Visual aura of migraine is usually harmless, but transient ischemic attack and seizure have health consequences
?Does Migraine Cause Hallucinations
How do I tell the difference between aura and stroke?
Strokes produce visual, sensory and/or speech symptoms almost instantaneously, and most frequently they are “negative” phenomena—that is, a loss of vision, numbness or weakness. Also with strokes, there is no sense of movement of the phenomena to other parts of the body. They don’t progress but are maximal at onset. Strokes usually are continuous and do not remit in one hour. A headache may or may not occur with a stroke. In addition, an aura occurring for the first time after the age of 40, with numerous vascular risk factors such as hypertension, diabetes and hyperlipidemia, should be investigated for transient ischemic attacks. If the visual symptom is ONLY negative (that is, a hemianopic scotoma), the person should be further investigated.
A migraine is a recurrent and severe headache which a whopping one in ten New Zealanders suffer from.
There are a few different types of migraines which people usually experience:
A classic migraine occurs in about 40% of migraine sufferers and has an aura (visual, auditory, olfactory or tactile).
A common migraine occurs in about 60% of migraine sufferers and has no aura.
A silent migraine is when a person experiences the aura, but no headache or pain afterwards.
A visual migraineis a silent migraine when the aura is visual.
A retinal migraineis very rare and its visual symptoms are the partial or total loss of vision, temporarily in one eye. In recurrent cases, it is most likely to affect the same eye each time. The vision fades out over five minutes, and can be described as a dimming of vision, flashes of light or patches of blank spots (scotomas) that enlarge to block out all sight in that eye. The vision returns to normal within an hour. This loss of vision is caused by reduced blood flow or spasms of the blood vessels in the retina or behind the eye, not in the brain.
Migraines might occur rarely, once or twice a year, or they could strike several times a month. The frequency differs drastically between sufferers and is often associated with an underlying cause. Migraines usually run in families as they have a genetic component. People with two parents who suffer from migraines have a 75% chance of having migraines themselves. Women are also three times more likely than men to get them.
BVD(Binocular vision dysfunction)and other binocular vision issues can have a huge impact on your life, both at work and at home, which is why it’s so important to understand what BVD is and the signs and symptoms to watch for.
In order for the eyes to work together as a team, they must be in perfect alignment. When they’re not, a number of unpleasant and sometimes painful physical symptoms can occur. Headaches, dizziness and balance issues are some of the most common indicators that BVD is present.
Other signs include:
Reading problems (losing your place frequently, skipping lines), as well difficulty comprehending what was read.
Severe light sensitivity and blurred/shadowed/doubled vision.
Anxiety and apprehension when in large, open indoor spaces with tall ceilings.
Treatment can include any of the following:
Custom micro-prism lensesthat help realign the eyes, thus greatly reducing or even eliminating the symptoms of BVD.
Prism contact lensesthat treat BVD, as well as contact lenses for astigmatism.[8]
Binocular vision dysfunction (BVD)is a visual condition where the line of sight from one eye tends to be slightly out of alignment with the line of sight from the other eye (usually vertical) and this puts heavy strain on the eye muscles as they are constantly trying to correct the alignment to achieve single focus vision.
The cause can be secondary to: normal facial asymmetry, acquired facial asymmetry from aging or head trauma from sports or injury damaging the nerves to your eye muscles causing the imbalance.
Binocular vision dysfunction means you see two images that compete in the middle where their fields of view overlap.
There are three forms of BVD:
1. Vertical Heterophoria 2. Superior Oblique Palsy 3. Horizontal misalignment
Symptoms of BVD
Those who suffer from Vertical Heterophoria or Superior Oblique Palsy tend to have a small amount of vertical eye misalignment, which the brain corrects by directing the eye muscles to properly reposition the eyes. However, using the eye muscles in this manner overworks them and they become strained and fatigued, causing the many symptoms of Vertical Heterophoria and Superior Oblique Palsy:
- Anxiety in crowds or large open spaces - Overly sensitive to light and glare - Double vision - Shadowed, overlapping or blurred vision - Skip lines or lose your place while reading. - Quickly fatigue while reading and difficulty with comprehension. - Closing or covering one eye to make it easier to see. - Headaches - Dizziness - Lightheadedness - Nausea - Anxiety - Motion sickness - Poor depth perception - Lack of good balance and drifting while walking - Poor coordination and Clumsiness - Aching eyes, especially with eye movement - Neck, upper back or shoulder pain - Head tilting [2]
There are a number of tests the doctor may perform to assess any difficulties with vision, including:
Developmental Eye Movement (DEM): Reading eye movements and assessing their accuracy. Sensory Fusion Assessment: This is a series of four separate examinations to discover if suppression, which can be part of an overall binocular vision disorder, is present. Near Point of Convergence (NPC): The test will find out if convergence and divergence dysfunctions are causing problems. Accommodative Convergence/Accommodation (AC/A): Any evidence of accommodation which exists is discovered by the results of this test. [4]
Binocular visionis vision in which creatures having two eyes use them together. The word binocular comes from two Latin roots, bini for double, and oculus for eye. According to Fahle (1987), having two eyes confers six advantages over having one.
It gives a creature a spare eye in case one is damaged.
It gives a wider field of view. For example, humans have a maximum horizontal field of view of approximately 190 degrees with two eyes, approximately 120 degrees of which makes up the binocular field of view (seen by both eyes) flanked by two uniocular fields (seen by only one eye) of approximately 40 degrees.
It can give stereopsis in which binocular disparity (or parallax) provided by the two eyes' different positions on the head gives precise depth perception. This also allows a creature to break the camouflage of another creature.
It allows the angles of the eyes' lines of sight, relative to each other (vergence), and those lines relative to a particular object (gaze angle) to be determined from the images in the two eyes.These properties are necessary for the third advantage.
It allows a creature to see more of, or all of, an object behind an obstacle. This advantage was pointed out by Leonardo da Vinci, who noted that a vertical column closer to the eyes than an object at which a creature is looking might block some of the object from the left eye but that part of the object might be visible to the right eye.
It gives binocular summation in which the ability to detect faint objects is enhanced.
Once the fields of view overlap, there is a potential for confusion between the left and right eye's image of the same object.
This can be dealt with in two ways:
one image can be suppressed, so that only the other is seen,
or the two images can be fused.
If two images of a single object are seen, this is known as double vision or diplopia.
Fusion of images (commonly referred to as 'binocular fusion') occurs only in a small volume of visual space around where the eyes are fixating. Running through the fixation point in the horizontal plane is a curved line for which objects there fall on corresponding retinal points in the two eyes. This line is called the empirical horizontal horopter. There is also an empirical vertical horopter, which is effectively tilted away from the eyes above the fixation point and towards the eyes below the fixation point. The horizontal and vertical horopters mark the centre of the volume of singleness of vision. Within this thin, curved volume, objects nearer and farther than the horopters are seen as single. The volume is known as Panum's fusional area (it's presumably called an area because it was measured by Panum only in the horizontal plane). Outside of Panum's fusional area (volume), double vision occurs. eResearch by Navid Ajamin -- spring 2016
When very different images are shown to the same retinal regions of the two eyes, perception settles on one for a few moments, then the other, then the first, and so on, for as long as one cares to look.
This alternation of perception between the images of the two eyes is called binocular rivalry.
When different images are shown to the two eyes, awareness can alternate such that each is intermittently suppressed and only one image is seen at a time. For instance, a picture of a girl can be shown to the left eye and a picture of a house to the right. Perception can then alternate - swapping between seeing the girl and the house. This phenomenon is called Binocular Rivalry.
Binocular Rivalry has generated broad interest as it permits an opportunity to explore the relationship between changes in conscious vision and brain activity in the absence of changes to sensory input. However, the function of binocular suppression remains a point of contention.[7]
Binocular rivalry is a phenomenon of visual perception in which perception alternates between different images presented to each eye.
Humans have limited capacity to process an image fully at one time. That is why the binocular rivalry occurs. Several factors can influence the duration of gaze on one of the two images. These factors include context, increasing of contrast, motion, spatial frequency, and inverted images. Recent studies have even shown that facial expressions can cause longer attention to a particular image. When an emotional facial expression is presented to one eye, and a neutral expression is presented to the other eye, the emotional face dominates the neutral face and even causes the neutral face to not been seen.
How do you fix an eye misalignment
Binocular depth perception arises as a consequence of the slightly displaced point of view of the two eyes. The horizontal displacement of image features in the two eyes (i.e. binocular disparities) makes it possible to reconstruct the depth relationships in the visual world.
The term depth perception refers to our ability to determine distances between objects and see the world in three dimensions. To do this accurately, one must have binocular stereoscopic vision, or stereopsis.
Depth perception is the ability to judge depth and distance. Depth perception requires binocular vision, but it may be assisted by monocular cues such as motion parallax, or how objects move in relation to the movement of the head; interposition, or object overlap; and color and contrast cues that suggest distance.
What causes depth perception problems?
There is not one answer, but in fact several conditions that can contribute to poor depth perception:
Strabismus – This is a condition where both of the eyes cannot be aligned simultaneously. One or both eyes may turn outwards, inwards, downwards, or upwards. This is commonly referred to as being cross-eyed.
Blurred vision – This is when one’s vision is not as sharp as normal and it makes it incredibly difficult to spot detail.
Amblyopia – This is a condition where one eye cannot focus as well as the other and is often called a “lazy eye.”
Eye trauma – Eye trauma is anything that disturbs or harms the eye. This prevents the eye or eyes from working as well as they should and can harm one’s vision.
Not everyone sees optimally. People suffering from amblyopia, optic nerve hypoplasia and strabismus often have reduced depth perception. A person with an injury to one eye, or a person missing one eye, may not be able to tell where objects are in relation to others. Visual therapy may help improve these problems.
Depth perception plays an important part in many activities. Driving, sewing, threading a needle, watching 3D movies and even walking on uneven ground all require certain levels of depth acuity. People without functioning stereoscopic vision may not be able to perform these activities or may struggle with them.
Two-eyed, or binocular vision, allows each eye to see from different angles. The brain processes the information coming from each eye and forms it into one image—a process called convergence. If binocular vision is working as it should be, the brain can interpret the information, which is called stereopsis. Those that have vision in only one eye usually have to rely on other cues to aid their depth perception.
Binocular matching of local features in the retinal images may be used to obtain estimates of the absolute disparity (and distance) of objects or surfaces, as well as the relative disparity (or relative distances) between different objects.
Other phenomena of binocular vision include:
utrocular discrimination (the ability to tell which of two eyes has been stimulated by light),
eye dominance (the habit of using one eye when aiming something, even if both eyes are open),
allelotropia(the averaging of the visual direction of objects viewed by each eye when both eyes are open),
binocular fusion or singleness of vision (seeing one object with both eyes despite each eye's having its own image of the object),and
binocular rivalry (seeing one eye's image alternating randomly with the other when each eye views images that are so different they cannot be fused).
When different images are presented to the two eyes, they compete for perceptual dominance, such that one image is visible while the other is suppressed. This binocular rivalry is thought to reflect competition between monocular neurons within the primary visual cortex. However, neurons whose activity correlates with perception during rivalry are found mainly in higher cortical areas, and respond to input from both eyes. Thus rivalry may involve competition between alternative perceptual interpretations at a higher level of analysis. To investigate this, we tested the effect of rapidly alternating the rival stimuli between the two eyes. Under these conditions, the perceptual alternations exhibit the same temporal dynamics as with static patterns, and a single phase of perceptual dominance can span multiple alternations of the stimuli. Thus neural representations of the two stimuli compete for visual awareness independently of the eye through which they reach the higher visual areas. This finding places binocular rivalry in the general category of multistable phenomena, such as ambiguous figures, and provides a new way to study the neural cause and resolution of perceptual ambiguities.
Binocular vision helps with performance skills such as catching, grasping, and locomotion.It also allows humans to walk over and around obstacles at greater speed and with more assurance.Orthoptists are eyecare professionals who fix binocular vision problems.[1]
Strabismus occurs when there are neurological or anatomical problems that interfere with the control and function of the extraocular muscles. The problem may originate in the muscles themselves, or in the nerves or vision centers in the brain that control binocular vision.
Grades of binocular vision
There are grades and methods of assessing binocular vision. The grades are the different steps in the development of stereopsis during the visual maturation. Testing of the grades is done by a synaptophore and graded as - no binocular single vision grade zero, simultaneous perception grade 1, fusion grade 2 and stereopsis grade 3. Limited form of testing can be done with worth four-dot test or Bagolini’s glasses.
The drawing at the left shows the view of two trees from the perspective of the eyes. The light green tree stands in front of the dark green tree. The right drawing shows a top view of the scene. When the eyes are focusing on the light tree, the image is projected on the fovea of the left and right eye. The angle between both projections is angle α. The images of the dark tree are projected on different positions of the peripheral retina in the left and right eye with angle ß. Because angle ß is smaller than angle α our brain interprets the dark tree as further away than the light tree. The size of the difference between α and ß represents the disparity. Large differences in angle indicate large differences in depth
Stereopsis is not present at birth but develops in the first months of life. That full-term and pre-term children develop stereopsis at the same age post-birth shows that the development depends on visual experience rather than biological maturation of the system.In the early months of life, we develop coarse stereopsis, which operates on high contrast lines and edges and enables us to align our eyes.
Four basic types of Da Vinci stereopsis cues
Alignment then permits the development of fusion and fine stereopsis. Fine stereopsis works over a much shorter range of disparities but enables us to make very fine depth judgments even in densely textured surfaces, such as grass or tree bark, where there are few or no depth cues monocularly.
important binocular visual skills:
- Tracking: the ability to move the eyes across a sheet of paper - Fusion: the ability to use both eyes together at the same time - Stereopis: binocular depth perception - Convergence: the ability of the eyes to move and work as a team - VisualMotorIntegration: the ability to transform images from a vertical to a horizontal plane[3]
Astigmatism(uh-STIG-muh-tiz-um) is a refractive error that prevents sufferers from seeing objects clearly from a distance or up close. Astigmatism may occur in varying degrees in each eye and can accompany myopia or hyperopia. Mildastigmatism is usually not noticeable, or causes only slight blurriness, while severe astigmatism causes objects to appear blurry at any distance. Approximately 80 percent of Americans have some degree of astigmatism, but many cases do not require correction.
In low-light conditions, blurry vision associated with astigmatism can become worse because when the lighting dims, your pupil dilates to let in more light.The more light that is let in, the more light that is scattered. This scattered light causes unfocused vision, as well as halos around bright lights and even night blindness.Bright headlights from oncoming and rear traffic can become particularly distorted, creating ‘lines’ of light around the headlight.
A normal cornea is shaped like a perfect sphere. The eye’s natural lens is also curved in equal degree in all directions. The corneas or lenses of people with astigmatism do not have equal curves. One side may be steeper than the other, making the cornea look more like a football than a basketball. Because of this, light entering the eye is not focused correctly on the retina, resulting in a blurred image.[1]
What are the signs and symptoms of astigmatism?
Signs and symptoms include:
Eyestrain
Squinting
Headaches
Difficulty driving at night
Distorted or blurred visionat all distances [5]
If you experience any of these symptoms, visit your eye care professional. If you wear glasses or contact lenses and still have these issues, a new prescription might be needed.
When to see a doctor
If your quality of vision detracts from your enjoyment of activities or interferes with your ability to perform everyday tasks, see an eye doctor. An eye doctor can determine whether you have astigmatism, and if so, to what degree. He or she can then advise you of your options to correct your vision.
If you're a healthy adult older than 40, have your eyes examined about every two to four years until age 55. After age 55, have them checked every one to three years for signs of eye disease or problems, and then every one to two years after age 65. If you have eye problems, such as astigmatism, you may need to have your eyes checked more frequently.If you're at risk of certain eye diseases, such as glaucoma, or you have diabetes, check with your doctor to see how often you need to have your eyes examined. Astigmatism occurs when your eyes are unable to focus light rays onto a single point, which is the ideal process. Usually this disorder causes blurry vision, possible sensitivity to light, eye discomfort and potentially headaches.
In astigmatism, the cornea has multiple powers, leading to multiple points of focus and blurry vision. People with astigmatism may also report double vision orghost images.
What are the types of astigmatism?
There are three types of of astigmatism: [11]
Lenticular astigmatism.
Affects the lens instead of the cornea. The lens allows the images to reach the retina, and this type of astigmatism makes it have variations.
Myopic astigmatism.
This type of astigmatism happens when astigmatism and nearsightedness are combined, causing the two curves to focus in front of the retina.
Hyperopic astigmatism.
This happens when farsightedness is combined with astigmatism, causing the two curves to focus behind the retina.
Mixed astigmatism.
When one eye is farsighted, while the other is nearsighted
Astigmatism can also be classified as regular or irregular:
Regular astigmatism means that the two curves are 90 degrees apart, while irregular astigmatism is not 90 degrees apart from each other.
Irregular astigmatism can be caused by an eye injury, eye trauma, surgery or an eye condition called keratoconus, which makes the cornea gradually thinner.
Tests anddiagnosis
To diagnose astigmatism, your eye doctor may:
Measure reflected light. By measuring light reflected from the surface of your cornea, a device known as a keratometer quantifies the amount and orientation of corneal astigmatism.
Measure the curvature of your cornea. Using light to project rings on to your cornea, a device called a keratoscope measures the amount of curvature to your cornea's surface and can confirm the presence of astigmatism. Observation through the keratoscope of the reflection of light from your cornea and inspection of the shape and spacing of the rings provide information about the degree of astigmatism.
To measure the change in corneal surface curvature, a process called corneal topography is used. Corneal topography uses a videokeratoscope, which is a keratoscope fitted with a video camera.[2]
Levels of Astigmatism
Astigmatism is measured in units of diopters. In a prescription, plus and minus signs in the ‘cylinder’ box indicate the astigmatism prescription, which is then followed by numbers indicating the location (axis) of astigmatism. Here is a rough breakdown of the different degrees of astigmatism:
0.25 to 0.75 diopters = mild astigmatism
1.00 to 2.50 diopters = moderate astigmatism
2.75 to 4.75 diopters = severe astigmatism
5.00 dioptersor higher = extreme astigmatism
To prescribe corrective wear for astigmatism, measurements are taken from a vertical and horizontal, or oblique approach, forming an axis. This is done because light enters the eye from different directions. Both the vertical and horizontal measurements will be different with astigmatism.
In general, higher levels of astigmatism show agreater disparitybetween two prescriptions, and with milder astigmatism, the values are much closer to each other.
Astigmatism in Children
The following are a few other abbreviationsyou may encounter on your eyeglass prescription:
SVD - Single Vision Distance, or glasses for distance only
SVN - Single Vision Near, or glasses for reading only
Sphere - Spherical power has the same power in all meridians
Cylinder - A cylinder power corrects astigmatism and represents the difference in the greatest power of the eye and weakest power of the eye, usually separated by 90 degrees.
Axis - indicates the angle (in degrees) between the two meridians of an astigmatic eye
PD - (pupillary distance, or distance between the centers of the two pupils between the eyes) This measurement is essential to designing glasses that comfortable to wear and optically perfect.
Prism - Prism is not commonly prescribed. It is often prescribed to displace the image in a certain direction for patients with crossed-eye (strabismus) or other eye muscle or focusing disorders.[3]
Diagnosis
Patients seek treatment because of blurred vision. A variety of tests can be used to detect astigmatism during the eye exam. The patient may be asked to describe the astigmatic dial, a series of lines that radiate outward from a center. People with astigmatism will see some of the lines more clearly than others.
Cover one eye with your hand, without pressing on the lid, and take the test.
Cover the other eye and begin the test again.If some of the lines appear grayer and some blacker, you probably have an astigmatism - consult your eye care specialist.
Simulation of the compensatory effect on chronic astigmatism when an image of a hydrangea is presented. The effect of the astigmatic blur and the automatic compensation were simulated for visualization purposes, according to the mechanisms of the adaptation model described in the Results and Methods sections. The edges of each image were detected with the Sobel operator (red). The edges are intact in the image of normal vision but severely biased vertically in the astigmatic retinal image. After being counterbalanced by the inversely biased edges of the automatic compensation, the vision with chronic astigmatism partly restores the original edges.
One diagnostic instrument used is the keratometer. This measures the curvature of the central cornea. It measures the amount and direction of the curvature. A corneal topographer can measure a larger area of the cornea. It can measure the central area and mid-periphery of the cornea. A keratoscope projects a series of concentric light rings onto the cornea. Misshapen areas of the cornea are revealed by noting areas of the light pattern that do not appear concentric on the cornea. eResearch by Navid Ajamin -- summer 2013
Because these instruments are measuring the cornea, it is also important to have a refraction in case the lens is also contributing to the astigmatism. The refraction measures the optics or visual status of the eye and the result is the eyeglass prescription. The refraction is when the patient is looking at an eye chart and the doctor is putting different lenses in front of the patient's eyes and asks which one looks better.
Proposed videokeratography pattern classification scheme. PSBT=prolate symmetric bow tie, PABT=prolate asymmetric bow tie, OSBT=oblate symmetric bow tie, OABT=oblate asymmetric bow tie, PI=prolate irregular, OI =oblate irregular, SF=steep/flat, LS=localised steep. Most of the patterns can be seen as a continuum, with some of them changing into different patterns (arrows) after manipulation of post-PKP astigmatism, by removal or adjustment of sutures. Blueand red colours imply flat and steep areas respectively, as in the conventional topographic map representation.[6]
Keratoconus (ker-uh-toe-KOH-nus) is a naturally occurring weakening of the cornea, characterized by its progressive asymmetric thinning and steepening. Keratoconus typically begins in the teens or 20s, progresses over a decade, and results in significant visual dysfunction, reduced quality of life, and permanent changes in the patient’s lifestyle.[7]
Keratoconus is an eye condition in which your cornea — the clear, dome-shaped front of your eye — gets thinner and gradually bulges outward into a cone shape.
Causes of Astigmatism [14]
How do I know which type of astigmatism I have
Astigmatism is primarily caused by irregularities in the shape of the cornea or lens of the eye. The specific causes can include:
Corneal Shape:Irregularities in the curvature of the cornea, such as a football-shaped cornea instead of a spherical one, can lead to astigmatism.
Lens Abnormalities: Changes in the shape of the eye's crystalline lens can also contribute to astigmatism.
Genetics: Astigmatism frequently has a hereditary component, which means that it can occur in families.
Eye Injuries or Surgeries: Trauma to the eye or certain eye surgeries can result in irregular astigmatism.
Keratoconus: A condition where the cornea progressively thins and bulges outward, leading to astigmatism.
Changes with Age: Astigmatism can develop or change as a person ages.
Eye Conditions: Certain eye conditions, such as corneal scars or degenerations, can cause irregular astigmatism.
Environmental Factors: Prolonged and intense use of the eyes for tasks like reading or computer work may contribute to eyestrain but is not a direct cause of astigmatism.
OCULUS PENTACAM. Refractive display of a patient with mild keratoconus. The upper left map (anterior curvature) shows nonorthogonal principal meridians, which is a hallmark of irregular astigmatism. The upper right (anterior elevation) and lower right (posterior elevation) show the classic positive island of elevation. The corneal thickness map (lower left) shows a moderately thinned cornea.
Treatment
Astigmatism can be treated by the use of cylindrical lenses. They can be in eyeglasses or contact lenses. The unit of measure describing the power of the lens system or lens is called the diopter (D). The lenses are shaped to counteract the shape of the sections of cornea that are causing the difficulty.
Correcting Astigmatism
Because the correction is in one direction, it is written in terms of the axis the correction is in. On a prescription, for example, it may say −1.00 × 180°. Cylinders correct astigmatism, minus spheres correct myopia, and plus spheres correct hyperopia.
There is some debate as to whether people with very small amounts of astigmatism should be treated. Generally, if visual acuity is good and the patient experiences no overt symptoms, treatment is not necessary. When treating larger amounts of astigmatism, or astigmatism for the first time, the doctor may not totally correct the astigmatism. The cylindrical correction in the eyeglasses may make the floor appear to tilt, thus making it difficult for the patient at first.
Generally, the doctor will place lenses in a trial frame to allow the patient to try the prescription at the exam. It may take a week or so to get used to the glasses, however, if the patient is having a problem they should contact their doctor, who might want to recheck the prescription.[4]
Convergence insufficiency occurs when your eyes don't turn inwardproperly while you're focusing on a nearby object. When you read or look at a close object, your eyes should converge — turn inward together to focus — so that they provide binocular vision and you see a single image. But if you have convergence insufficiency, you won't be able to move your eyes inward to focus normally.
Convergence insufficiency is caused by complications coronating eye movements and muscles. Instead of the eyes coming together (converging) to focus on objects close by, one or both eyes point outward. Because the brain controls all eye movement, damage to the brain is the leading cause of convergence insufficiency. However, the exact cause of this condition remains a mystery. The working theory among researchers is that neurogenerative disease such as Parkinson’s disease, myasthenia gravis and Alzheimer’s disease in some way cause CI.
Convergence insufficiency (CI) is a common eye condition that affects the ability of the eyes to work together. This condition occurs when the eyes are unable to converge or move inward effectively, making it difficult to focus on objects that are close up. This can cause a variety of symptoms, including eye strain, headaches, blurred vision, and difficulty reading.
Symptoms
Not everyone with convergence insufficiency experiences symptoms. Signs and symptoms occur while you're reading or doing other close work and may include:
Tired, sore or uncomfortable eyes (eyestrain)
Headaches
Blurred vision
Difficulty reading — words seem to float on the page, you lose your place or you read slowly
Double vision
Difficulty concentrating
A "pulling" feeling around your eyes
Sleepiness
Squinting, rubbing or closing one eye
Trouble concentrating. It can be difficult to focus and pay attention. In school, children may do work slowly or avoid reading, which can affect learning.
If you or your child experiences symptoms of convergence insufficiency or has problems reading, consult an eye care professional, such as an ophthalmologist or an optometrist. A technician called an orthoptist may assist the eye care professional in evaluating and treating convergence insufficiency.
Convergence insufficiency results from misalignment of the eyes when focusing on nearby objects. The exact cause isn't known, but the misalignment involves the muscles that move the eye. Typically, one eye drifts outward when you're focusing on a word or object at close range.
Complications
Difficulties with reading and concentrating can adversely affect a child's learning. Convergence insufficiency typically isn't detected in routine eye exams or school-based vision screenings. A child with the condition may be evaluated for learning disabilities because of his or her reading troubles.
Tests and diagnosis
People with convergence insufficiency may have otherwise normal or "20-20" vision, and the condition may not be detected during a routine eye exam. To diagnose convergence insufficiency, your eye doctor may do the following, including special eye-focusing tests:
Treatments and drugs
If convergence insufficiency isn't causing symptoms, you generally don't need treatment. But for people with symptoms, treatment with eye-focusing exercises can increase the eyes' convergence ability. Treatment may take place in the office of a trained therapist or at your home.
Treatments may include:
A study sponsored by the National Eye Institute of the National Institutes of Health compared home-based treatment with doctor office-based treatment for convergence insufficiency in children ages 9 to 17. Study results showed that the most effective therapy was a weekly hourlong session of in-office vision therapy with at-home reinforcement exercises. Other studies have also found that office-based treatment is effective about 75 percent of the time.
Home-based treatment with pencil pushups or computer programs hasn't been shown to be as effective — in some studies, it works only about one-third of the time. But home treatment costs less and is more convenient. Only a small percentage of eye care providers offer in-office therapy for convergence insufficiency. Many people who can't find or can't afford in-office therapy opt for home-based treatment.
If you choose home treatment, many experts recommend using computer software programs along with pencil pushups. The combined approach may be more effective, and the computer therapy is more engaging for children.
Treatment for convergence insufficiency may take three months or longer, though you'll likely start to see improvement in your symptoms after four weeks. After your convergence ability has improved, you can help maintain your improved vision by continuing to read and do other near tasks. Treatment can permanently cure convergence insufficiency, but symptoms may come back after an illness, lack of sleep or when you're doing a lot of reading or other close work. In rare cases, eye-focusing exercises don't work and your doctor may recommend surgery.
eResearch by Navid Ajamin -- spring 2013
Take a medical history. This may include questions about problems you have with focusing, blurred or double vision, headaches, and other signs and symptoms.
Vision Therapy for Convergence Insufficiency
Measure the near point of convergence (NPC). This test measures the distance from your eyes to where both eyes can focus without double vision. For this simple test, the examiner holds a small target, such as a glass ball, printed card or penlight, in front of you and slowly moves it closer to you until either you experience double vision or the examiner recognizes that your eyes can no longer focus together.
Assess positive fusional vergence (PFV). During this test, you're asked to read letters on an eye chart while looking through prism lenses. The examiner will note when you begin to have double vision.
Perform a routine eye exam. If you have any other vision problems, such as nearsightedness, your ophthalmologist or optometrist may conduct tests to assess the degree of the problem.
Pencil pushups. In this simple exercise, you focus on a small letter on the side of a pencil as you move it closer to the bridge of your nose, stopping the movement if you have double vision. The exercise is often done for 15 minutes a day, five or more days a week.
Computer vision therapy. Eye-focusing exercises are done on a computer using special software designed to improve convergence. You may print out the results to share with your eye doctor.
Reading glasses. Glasses with built-in prisms force your eyes to work harder to align and are sometimes used for people who need help with their reading vision. But they can be tiring to your eyes and generally haven't proved effective.
Your brain controls all your eye movements. When you look at a nearby object, your eyes move inward to focus on it. This coordinated movement is called convergence. It helps you do close work like reading or using a phone.
Convergence insufficiency is a problem with this movement. The condition causes one or both eyes to drift outward when you look at something close by.
Doctors don’t know what causes convergence insufficiency. However, it’s associated with conditions that affect the brain.
These may include:
traumatic brain injury
concussion
Parkinson’s disease
Alzheimer’s disease
Graves’ disease
myasthenia gravis
Convergence insufficiency appears to run in families. If you have a relative with convergence insufficiency, you’re more likely to have it, too.
Your risk is also higher if you use the computer for long periods of time. Diagnosing convergence insufficiency
It’s common for convergence insufficiency to go undiagnosed. That’s because you can have normal vision with the condition, so you can pass a normal eye chart exam. Plus, school-based eye exams aren’t enough to diagnose convergence insufficiency in children.
You’ll need a comprehensive eye exam instead. An ophthalmologist, optometrist, or orthoptist can diagnose convergence insufficiency.
Visit one of these doctors if you are experiencing reading or visual problems. Your child should also see an eye doctor if they’re struggling with schoolwork.
At your appointment, your doctor will do different tests.
They might:
Ask about your medical history. This helps your doctor understand your symptoms. Perform a full eye exam. Your doctor will check how your eyes move separately and together. Measure near point of convergence. Near point convergence is the distance you can use both eyes without seeing double. To measure it, your doctor will slowly move a penlight or printed card toward your nose until you see double or an eye moves outward. Determine positive fusional vergence. You’ll look through a prism lens and read letters on a chart. Your doctor will note when you see double.
Vision Exams
Following symptom analysis, a comprehensive vision exam is vital. These exams are not just about checking visual acuity; they involve a series of tests specifically designed to evaluate the eyes’ ability to converge when focusing on close objects. Key tests include:
Cover Test: Determines how the eyes move and work together.
Near Point of Convergence (NPC): Measures the closest point at which the eyes can focus together without double vision.
Positive Fusional Vergence (PFV) at Near: Assesses the ability to sustain focus on a close target without experiencing double vision or discomfort.
Can you see clearly now? Probably not — changes in your vision during pregnancy often stick around until after you deliver.
What blurred vision during pregnancy is ?
Difficulty with your vision and dry, irritated eyes are common pregnancy symptoms.
Blurry vision during pregnancy is a temporary change in the quality of your eyesight. It occurs due to the effects of hormone changes on your eyes. Unexpected changes to your vision can be worrisome. But blurry vision is rarely a sign of a permanent eye issue.
What causesblurred vision pregnancy ?
Pregnancy hormones (what else?) that decrease tear production (ironically, since they certainly don't decrease crying!), leading to eye dryness, irritation, and discomfort. Hormones also cause fluid buildup in your eyes, the same way they make you have swollen ankles and feet. This can lead to changes in the curvature of your eye, which causes a change in your vision during pregnancy.
What you need to know about blurred vision pregnancy
Changes in vision are normal for many women during pregnancy. You might not see as well, or your contact lenses might feel less comfortable. Luckily, these changes are temporary and your vision should go back to normal after delivery. Remember, however, that some serious vision problems can be a sign of gestational diabetes or high blood pressure, so be sure to mention any vision changes to your practitioner. eResearch by Navid Ajamin -- spring 2013
What to do about blurred vision pregnancy
If you wear glasses or contacts, don't bother with a new prescription until after you've had your baby.
If your contacts are bothering you, consider wearing your glasses until after delivery, or use lubricating drops recommended by your eye doctor if your eyes feel especially dry. (You can use drops even if you don't wear contacts.)
Steer clear of corrective eye surgery six months before conceiving, during pregnancy, and for six months after delivery, according to ophthalmologists. It won't hurt your baby, but it might lead to over-correction, which could require another surgery later on.
If you notice blurring, dimming vision, spots, and floaters that don't go away, or double vision that persists for more than two hours, call your practitioner.
Which hormones affect our eyes?
Everyone experiences hormonal changes throughout their lives, and these changes affect all parts of your body, including your eyes.
Sex hormones (namely estrogen) are the hormones most likely to affect our eyes and our vision. In particular, they play a big part in how dry or moist our eyes are and feel.
There are sex hormone receptors in our conjunctival goblet cells, lacrimal glands and meibomian glands. These three sites are responsible for making the three major components of our tears. These three components make up the three different layers of our tear film (oil layer, aqueous-watery layer and mucus layer). Disruption to one or more of these layers can result in dry eye symptoms.
Hormonal changes during puberty
During puberty, the large influx of hormones causes many changes in children. As their arms and legs lengthen, so do their eyeballs! A lengthening eyeball can result in blurry vision and myopia, or short-sightedness.
Myopia can be corrected with spectacles or contact lenses. And once the eyes have stopped changing, myopia can also be corrected with laser vision correction surgery.
There are techniques and treatments available to prevent or reduce this eyeball lengthening. This area of health care is referred to as Myopia Management or Myopia Control. The benefit of slowing down this growth-related change is that it could reduce how myopic a child or young adult may become. The more myopic a person is, the higher their risk of developing eye disease and loss of vision. So by reducing the level of myopia in an individual, we can reduce their risk of developing sight-threatening conditions later in life.
Young, pregnant woman complains of 'smudge' in vision
Hormonal changes in adult women
Women experience significant hormonal changes during pregnancy, breastfeeding, menopause and while on birth control medication. The hormones most involved are estrogen and progesterone.
Their changing levels can affect the eye’s oil glands, which can lead to dryness. Estrogen can also make the cornea less stiff with more elasticity, which can affect how light travels into the eye. The dryness and the change in refraction can cause blurry vision and can also make wearing contact lenses difficult.
Pregnancy and breastfeeding
If you are breastfeeding, you may also experience some moving specks and lines, or floaters, in your vision.
In addition, you can have eye puffiness, which impacts your peripheral vision.
With the changes that occur during pregnancy, women may experience blurry vision, light sensitivity, and even headaches and migraines due to fluctuating hormone levels and fluid retention. Most women’s vision will return to normal after giving birth and once breastfeeding has stopped.
However, if your vision doesn’t return to normal a couple of months after pregnancy, or it changes suddenly or drastically, seek medical advice sooner. It could be due to a more serious medical condition like diabetes or hypertension (high blood pressure).
Perimenopause and menopause
The hormonal shifts associated with perimenopause and menopause can also trigger vision changes.
Menopause occurs due to a drop in estrogen levels. This results in a drying out of tissues (skin, mucosal membranes, and hair). As tissues dry their structure can also change. This can affect vision by drying out the outer surfaces of the eye. A dry eye is a swollen eye and can lead to physical discomfort, contact lens intolerance, pain and blurred vision.
Menopause tends to occur in women aged 45 to 55 years of age, but perimenopause can begin a few months or a few years before that.
Menstruation
Although less common, some menstruating individuals may detect changes to their vision and eyes during the first week of menstruation. This correlates to an influx of estrogen at the beginning of the cycle which can cause blurred vision, trouble focusing, and watery eyes.
The dry eye that occurs as a result of hormonal changes can be treated. Artificial tears or lubricating eye drops are usually enough to resolve most people’s issues. Occasionally more involved treatments are required. But talking to your GP about ways to adjust your hormone levels medically, should have a positive impact on dry eye symptoms.
Thyroid Hormones and Vision
Your infant's vision development
Thyroid hormones play a crucial role during the body’s development, including the development of the eyes. The thyroid gland is located at the base of our neck. It uses iodine from our food to produce two hormones: triiodothyronine (T3) and thyroxine (T4).
Thyroid eye disease develops when the body’s thyroid gland does not produce the correct amount or type of hormones.
One thyroid-related condition, called Graves’ disease, develops when there is an overproduction of thyroid hormones. About 30% of people with Grave’s disease also have eye-related changes such as; bulging eyes, puffy or retracted eyelids, light sensitivity, double vision, loss of vision, gritty, red or painful eyes.
Abnormal thyroid hormone levels can impact other aspects of eye development and disease.
Research has shown that people with higher levels of thyroxine (T4) are at increased risk of having age-related macular degeneration (AMD) and other retinal changes. And in another study, thyroid hormone levels appear to affect the ongoing development and regulation of the eye’s cones (cells responsible for your colour vision).
Male Hormones and Vision
Androgens are a group of hormones that control some male traits and reproductive activity. Testosterone and androstenedione are both androgens. Androgens are present in both males and females, even though they are often considered ‘male hormones’.
For example, women with polycystic ovary syndrome (PCOS) often have dry eyes due to excess androgen levels.
Androgens positively promote the function of meibomian glands and lacrimal glands. Meibomian glands make oil that prevents tears from evaporating, and the lacrimal glands produce the watery layer of our tears. So a drop in androgens can cause dry eyes by altering two important layers of the tear film.
Androgen levels drop with age, for both males and females. By the age of 50 years, it has dropped by about 30%, which is why dry eyes are more common as we age. Meibomian Gland Dysfunction is one of the most common causes of dry eye.
Is it normal to see flashes in your vision while pregnant?
During pregnancy it is possible that you'll observe flashing lights or blind spots. A condition known as migraine headache with aura, which some women encounter for the first time during pregnancy, is one possible cause. An aura precedes a painful headache (typically on one side of the head) with this syndrome.
Can pregnancy cause dizziness and vision changes?
Vision changes like blurred vision occur frequently during early pregnancy, as your body is flooded with hormones, fluid levels increase, and the body adapts to the changes of pregnancy. Blurry vision may be accompanied by morning sickness symptoms, like nausea, dizziness, and vomiting.
Can low iron cause blurry vision in pregnancy?
There is no evidence that low iron causes blurred vision. However, low iron can cause retinal changes leading to anemic retinopathy. Eye symptoms of low iron can include a pale coloring of the inside of the lower eyelids.
Why does preeclampsia cause blurred vision?
Vision changes in pregnancies complicated by preeclampsia can be caused by intraocular pathology, cortical changes, and medical therapy. Although vision often returns to baseline, retinal abnormalities and white matter lesions can develop during preeclampsia and persist, sometimes even many years after giving birth.
Is it normal to have blurry vision after pregnancy?
Women may undergo vision changes throughout pregnancy and into the postpartum period. These changes are usually mild and temporary myopic changes that resolve after the body returns to its pre-pregnancy state.
نام دیگردو بینیدیپلوپیا است که در آن از یک شی دو تصویر دیده می شود.
به طور کلی دو نوع دوبینی وجود دارد:
دوبینیتکچشمی
دوبینیدوچشمی
زمانی که یک بیمار با نا رضایتی از دوبینی مراجعه می کند ابتدا باید مشخص شود:
1- در کجا دو تصویر از هم فاصله گرفته اند و در کجا در هم رفته اند.
2- آیا به صورت افقی یا عمودی از هم جداشده اند. اگرچه بیشتر شکایات دوبینی درنتیجه مشکلات دید دوچشمی است، اما از دلایل احتمالی دیگراین مشکل می توان به عیب انکساری اصلاح نشده و دوبینی تک چشمی اشاره نمود. درعیب انکسار اصلاح نشده ممکن است بیمار بیان کند که دو تصویر به طور کامل از هم جدا نیستند و تمایل به ادغام شدن دارند. ممکن است در این حالت شکایت بیمار به دلیل آستیگمات اصلاح نشده یا حتی دوبینی اصلاح نشده ای باشد که با تطابق اصلاح نمی شود و یا ممکن است پیر چشمی باشد.
دوبینی تک چشمی(monocular diplopia)
به دوبینی گویند که تنها در یک چشم وجود دارد. این دوبینی حتی زمانی که چشم دیگر بسته است ادامه می یابد و زمانی که فرد به جهت دیگری نگاه می کند هم این دوبینی از بین نمی رود.اگر حدس زده شود که دلیل شکایت بیمار از دوبینی، دوبینی تک چشمی باشد باید از بیمار سوال شود که آیا وقتی یک چشم بسته است این اتفاق می افتد؟ دلایل کلاسیک برای دوبینی تک چشمی قوز قرنیه است. بیمار با کراتوکونوس علاوه بر دوبینی تک چشمی از آزار و ضعف بینایی در حین استفاده از عینک مشکل دارد.
از علائم کلینیکی قوز قرنیه می توان به موارد زیر اشاره نمود:
نازک بودن و برجستگی راس قرنیه که با اسلیت لمپ مشاهده می شود و انحنای زیادی که در کراتومتری دیده می شود و در رتینوسکوپی رفله نور به صورت موج دار است.زمانی که بیمار به پایین نگاه می کند برجستگی های قرنیه ممکن است به صورت دندانهای در پلک پایین دیده شود. دوبینی تک چشمی می تواند در اثر عوامل زیر ایجاد شود:
آستیگماتیسم
کراتوکونوس (قوز قرنیه)
ناخنک (pterygium): ضخیم شدگی در ملتحمه، لایه موکوسی که سطح داخلی پلکها و قسمت سفید چشم را می پوشاند. این ضخیم شدگی به سمت قرنیه افزایش می یابد.
کاتاراکت: شفافیت لنز به مقدار زیادی کاهش می یابد. از جمله ریسک فاکتورهای آن می توان به این موارد اشاره کرد:سن بالای 65 سال، تروما یا ضربه به چشم، دیابت طولانی مدت، سیگار کشیدن، استفاده از داروهای استروئیدی و یا استفاده از درمانهای رادیولوژی
جابه جایی لنز: لیگامان یا رباطی که به لنز متصل است و آنرا نگه می دارد، پاره می شود و لنز جابه جا می گردد.دلیل این اتفاق می تواند ترومای چشم و یا حالتی باشد که سندروم مارفان نامیده می شود.
خشکی چشم
بعضی از مشکلات رتین: زمانی که سطح رتین کاملا صاف نباشد (که دلایل مختلفی دارد) ممکن است دوبینی تک چشمی ایجاد گردد.
چند مردمکی بودن
Causes of Binocular Double Vision
‘Strabismus’ or ‘Squint’ is considered to be one of the most common causes of double vision – a condition, which disturbs the alignment of the eyes. It is commonly found in children. However, the presence of strabismus doesn’t always lead to diplopia.
Other conditions leading to diplopia can include:
Thyroid Issues: Located in the neck region, one of the functions of the thyroid gland involves producing a hormone named ‘thyroxine’. The external muscles controlling the eye can undergo various changes due to thyroid malfunction, which include “Grave’s Ophthalmopathy” – a condition leading to the protruding of the eyes because of fat and tissue build-up behind them.
Stroke or Transient Ischemic Attack (TIA): One of the major implications of a stroke is the inability of blood to reach the brain, also affecting the nerves controlling the eye muscles, possibly leading to double vision.
Aneurysm: A condition leading to a bulge in a blood vessel inside the brain, which can lead to extra pressure on the nerve of the eye muscle, turning into a possible reason for double vision.
Diabetes: It can not only affect the blood vessels supplying blood to the retina at the back of the eye, but also the nerves responsible for controlling the movement of the eye muscles.
Myasthenia Gravis: Muscle weakness is one of the major symptoms of myasthenia gravis, also including the ones needed to control eyes.
Brain Tumors: A tumor in the brain can create a growth behind the eye, which can sometime inflict damage upon the optic nerve, possibly hindering with the free movement of the eyes.
Multiple Sclerosis: Also referred as ‘MS’, this disease involves damage to the central nervous system, which also includes nerves in the eyes.
Head Injury: Any type of physical damage to the brain including muscles, nerves or sockets of the eyes can cause issues in the movement of the eyes, a possible cause of double vision.
Causes of Monocular Double Vision
The presence of double vision in only one eye is referred as ‘monocular double vision’ –relatively less common than binocular diplopia.
It can be caused by the following reasons:
Abnormalities of the iris, lens, or fluid within the eye[9]
Astigmatism: It can cause monocular double vision because it leads to an irregularly shaped cornea with two curves on the surface, more like a football, while it should be perfectly round like a basketball.
Dry Eye: When your eye is unable to produce enough tears, or tears start drying too quickly, your susceptibility for double vision increases.
Keratoconus: Due to this degenerative eye condition, cornea becomes too thin and cone-shaped, increasing your risks of diplopia.
Retinal Abnormalities: For example, macular degeneration, which slowly fades out the central vision of a person, also producing a swelling sometimes, leading to double vision in one eye in most of the cases.
Cataracts: More than half of the population of the U.S over 80 ends up with cataracts, sometimes also causing diplopia in one eye.
Diagnosis eResearch by Navid Ajamin -- autumn 2012
Diplopia or double vision is a visual impairment consisting in perceiving two images of the same object. It can be horizontal, vertical or diagonal, depending on the place where the dual images appear (beside, below, above or diagonally with regard to the object).
There are also different types of strabismus that can cause double vision:
Oculomotor nerve palsy
Strabismus that appears after eye surgery
Orbital trauma
Thyroid disorders
Some forms of child strabismus that last into adulthood
Strabismus of the myopic patient
Neurological diseases (such as myasthenia gravis)
Sensory strabismus (occurs when one of the two eyes has very low vision)[4]
Other disorders associated with strabismus in children include:[5]
Apert syndrome
Cerebral palsy
Congenital rubella
Hemangioma near the eye during infancy
Incontinentia pigmenti syndrome
Noonan syndrome
Prader-Willi syndrome
Retinopathy of prematurity
Retinoblastoma
Traumatic brain injury
Trisomy 18 (Edwards’ syndrome)
Strabismus that develops in adults can be caused by:
Botulism
Diabetes (causes a condition known as acquired paralytic strabismus)
Graves disease
Guillain-Barré syndrome
Injury to the eye
Shellfish poisoning
Stroke
Traumatic brain injury
Vision loss from any eye disease or injury
اغلب اوقات پی بردن به دوبینی در بزرگسالان ساده است، چون آنها می توانند آنچه را که می بینند توصیف کنند. تشخیص در کودکان سخت تر است چون نمی توانند توصیف خوبی از دیده های خود ارائه دهند. والدین این کودکان ممکن است متوجه شده باشند که کودکشان لوچ است، یا چشمش را با یک دستش می پوشاند، سر خود را به صورت غیر نرمال کج می کند و یا از پهلو نگاه می کند.
مشکلات دید دوچشمی
اگر دوبینی تنها گاهی اوقات اتفاق بیفتد، ممکن است بیمار متوجه شود که برای فواصل دور یا نزدیک و یا هر دو مقدار انحراف دارد؛ به طور مثال بیماری که انحراف زیادی دارد ممکن است برای انجام اعمال و وظایفش در فواصل دور(مثل رانندگی) دوبینی گهگاهی را تجربه کرده باشد. یا بیماری که دچار نقص در سیستم تقارب خود است ممکن است از دوبینی به دنبال کار نزدیک طولانی مدت شکایت کند. اگر فرد دوبینی گهگاهی عمدی را تجربه کند، ممکن است دلیل آن فوریا عمودی همرا با فیوژن عمودی ناکافی باشد.
بیماران با سابقه استرابیسم به ندرت از دوبینی شکایت دارند، چون قبلا از طریق ساپرس کردن، فیکسیشن خارج از مرکز،آمبیلوپی و یا مجموعه ای از این ها، با این وضعیت سازگاری پیدا کرده اند.به هر حال اگر دوبینی اخیرا شروع شده باشد احتمال فلج شدن ماهیچه وجود دارد. در بیماران مسن باید توجه ویژه ای به احتمالات اجزاء عمودی دوبینی کرد: احتمالا علت دو بینی پارگی رگهای مغزی مثل پاره شدن حلقه ولیس باشد.
دوبینی متقاطع و غیر متقاطع
معمولا افرادی که به طرفین انحراف دارند (Lateral phoria) زمانی که چشم ها از هم جدا می شوند ممکن است دوبینی متقاطع یا غیر متقاطع را تجربه کنند. برای درک مفهوم دوبینی متقاطع از غیر متقاطع لازم است رابطه ی بین میدان بینایی و تصویر رتینال را بشناسیم؛ که این رابطه عبارت است از: تصویر اشیاء موجود در سمت راست میدان بینایی، سمت چپ رتین و تصویر اشیاء سمت چپ میدان بینایی سمت راست رتین تشکیل می شود.
در افرادی که اگزوفوریا دارند تصویر جسمی که باید بر روی فووا دو چشم تشکیل شود، مثلا در چشم راست آنها این تصویر، سمت راست فووا تشکیل می شود و فرد تصور می کند که شیء در سمت چپ میدان بینایی اش قرار دارد؛ یعنی فرد دو تصویر می بیند. تصویری که توسط چشم راست دریافت می شود سمت چپ تصویر چشم چپ دیده می شود. در نتیجه دوبینی که رخ می دهد از نوع متقاطع است.
در بیمارانی که ایزوفوریا دارند تصویر شیء مورد نظر سمت چپ فووا چشم راست تشکیل می شود؛ پس تصویری که توسط چشم راست درک می شود سمت راست تصویری است که توسط چشم چپ درک می شود. در نتیجه دوبینی غیر متقاطع بوجود می آید.
مدت زمان مورد انتظار (Expected duration)
این که چه مدت دوبینی ادامه می یابد بستگی به علت ایجاد کننده آن دارد. به طور مثال کاتاراکت و ناخنک ممکن است در طول زمان بدتر شوند؛ ولی هر دو می توانند از طریق عمل جراحی تصحیح شوند. در فردی که دوبینی وی به علت دیابت است، اعصاب اغلب بعد از چند ماه دوباره رشد می کنند. زمانی که این دو اتفاق می افتد دوبینی تقریبا ناپدید می شود. بچه هایی که به دلیل استرابیسم دچار دوبینی شده اند، با درمان استرابیسم، دوبینی آنها بهبود می یابد.
درمان (Treatment)
درمان دوبینی بستگی به دلایل ایجاد کننده آن دارد. برای مثال در افرادی که آستیگمات باعث دوبینی آنها شده می توان از کنتاکت لنزهای ویژه استفاده نمود. گاهی اوقات به راحتی می توان با به روز کردن عینک تجویز شده از بروز مشکلات جلوگیری کرد. برای درمان کاتاراکت و ناخنک از جراحی استفاده می شود. همچنین جراحی بر روی ماهیچه ها نوع خاصی از دوبینی را درمان می کند. اغلب در این جراحی ها از بخیه هایی قابل تنظیم استفاده می شود که وضعیت چشم ها چند ساعت پس از جراحی هماهنگ شود. همچنین می توان با به کار بردن منشور در عینک تجویزی، تصویری که توسط یک چشم ایجاد می شود با تصویر چشم دیگر را هماهنگ کردن و منطبق کردن کرد. برای کودکانی که استرابیسم دارند .
درمان شامل: پوشاندن عینک تجویز شده، پریزم درمانی برای مرتب کردن چشم ها در یک ردیف، ویا جراحی است.دوبینی ایجاد شده بر اثر داروهای شیمیایی یا عصبی ممکن است یا درمان ان بیماری بهبود یابد. تزریق بوتولینم می تواند ماهیچه های قوی تر را تضعیف کند تا با هماهنگ شدن با ماهیچه های ضعیفتر یک بالانس بینایی ایجاد شود.اولین تستی که از بچه ها گرفته می شود باید قبل از 6 ماهگی و همراه با تست های follow up در سنین 3 سالگی باشد. افراد مسن تر از 40 سال حتی اگر مشکل بینایی قابل توجهی هم نداشته باشند، باید هر دو سال یک بار چک شوند.
تست میدان دوبینی
در تست broad H ، اگر چشمی در هر یک از حرکات میدان، نسبت به چشم دیگر تاخیر داشته باشد، از بیمار می خواهیم یک جفت عینک RED-GREEN بزند (لنز قرمز روی چشم راست!). در حالی که تست broad H (H پهن و عریض) تکرار می شود از بیمار می خواهیم گزارش کند که آیا 2 نور (یکی قرمز و دیگری سبز) در دو میدان دید با نگاه ثابت و خیره دیده می شوند یا نه؟! و اگر چنین است چه میزان فاصله بین دو تا نور وجود دارد. فرض می کنیم که بیمار گزارش کرد دوبنی در قسمت تحتانی سمت چپ میدان دید وی وجود دارد و نور سبز نسبت به نور قرمز در سمت پریفرال تری قرار می گیرد. ماهیچه مستقیم با همان نام برای سمت چپ تحتانی میدان، L.I.R (Left Inferior Rectus) نام دارد. در حالی که ماهیچه مایل با نام مخالف برای آن قسمت میدان R.S.O (Right Superior Oblique) می باشد.چون بیشترین تصویر پریفرال مربوط به چشم چپ (تصویر سبز رنگ) می شود، L.I.R ماهیچه معیوب می باشد. [1]
BINOCULAR DIPLOPIA
Double vision can occur when the two eyes are not correctly aligned while aiming at an object, such as in esotropia and exotropia - these result in uncrossed diplopia and crossed diplopia, respectively (i.e. "crossed eyes", in esotropia, result in uncrossed diplopia). When the eyes are misaligned and aimed at different targets, two non-matching images are sent to the viewer's brain. When the viewer's brain accepts and uses two non-matching images simultaneously, double vision results.
Can astigmatism cause double vision
Double vision is dangerous to survival, therefore, the brain naturally guards against its occurrence. In an attempt to avoid double vision, the brain can ignore one eye (suppression). Due to the brain's ability to suppress one eye, double vision can appear to go away without medical evaluation or treatment. The causes of the double vision are very likely still present and loss of vision in one eye can occur due to lack of treatment. The loss of vision in one eye can be temporary or permanent depending on detection and treatment. It is in this way, that diplopia contributes to loss of depth perception and binocular vision, amblyopia (lazy eye), and/or strabismus (deviating eye).
MONOCULAR DIPLOPIA
Diplopia can also occur when viewing with only one eye; this is called monocular diplopia, or where the patient perceives more than two images, monocular polyopia. In this case, the multiple vision can be caused by a structural defect in the vision system, such as cataracts, subluxation of the crystalline lens or Keratoconus causing irregularities in the refraction of light within the eye.
TEMPORARY DIPLOPIA Temporary diplopia can also be caused by intoxication from alcohol or head injuries, such as concussion. If temporary double vision does not resolve quickly, one should see an eye doctor immediately. It can also be a side effect of the anti-epileptic drugs Phenytoin and Zonisamide.[2]
Example of palinopsia. An example of a moving object (the hand is moving from left to right) with perseverance of multiple images is shown.Palinopsia (Greek: palin for "again" and opsia for "seeing") is the persistent recurrence of a visual image after the stimulus has been removed. Palinopsia is not a diagnosis, it is a diverse group of pathological visual symptoms with a wide variety of causes.[7]
Causes
Diplopia has a diverse range of ophthalmologic, infectious, autoimmune, neurological, and neoplastic causes.
Damage to the third, fourth, or sixth cranial nerves, which control eye movements.
Cancer ;Trauma ;Diabetes ;Migraine ;Multiple sclerosis ;Fluoroquinolone antibiotics
Spectacles with optical lenses can help correct double vision.
Depending on the cause, the treatments for binocular vision vary, but they include:
wearing glasses
eye exercises
wearing an opaque contact lens
botulinum toxin (Botox) injections into the eye muscles, causing them to remain relaxed
wearing an eye patch
surgery on the muscles of the eye to correct their positioning
A stick-on prism, placed between the eyes at the center of the spectacle frame, can also help to realign the images from each eye.
Eye exercises
Exercises cannot treat many of the conditions that cause double vision. However, some exercises can help with convergence insufficiency.
Smooth convergence
Focus on a detailed target, perhaps a thin stick or small text in a magazine.
Hold this at eye-level, an arm’s length away from you.
Aim for the image to remain as a single image for as long as possible.
Move the target towards the nose in a slow, steady fashion.
When the single image becomes two images, your eyes have stopped collaborating. Focus intensely on bringing these images back together. Once they join, bring the target closer to the nose.
Once you become unable to rejoin the images, move your hand back to its original position and start the exercise again.
The normal convergence range is 10 centimeters (cm) away from the nose. Aim to keep the image as a single image up to the 10cm mark.
An orthoptist may provide a tool known as a Dot Card to assist these steps.
Jump convergence
Choose a similar target to that in the smooth convergence exercise.
Start the target at a 20 cm distance from the nose.
Fix your gaze on the target for between 5 and 6 seconds.
Switch to looking at a fixed object around 3 meters (m) away for around 2 to 3 seconds.
Switch your vision back at the nearer target.
Repeat this, gradually moving the target closer, until you can focus on the object when it is 10 cm away without double vision.
The effectiveness of these exercises is largely restricted to treating convergence insufficiency.
If symptoms do not improve, visit a doctor for further testing.
در صورتيكه شما به بيماري ديابت مبتلا هستيد بدن شما نميتواند بدرستي از قند استفاده و آنرا ذخيره كند. ديابت باعث افزايش قند خون، عطش بيش از حد و تكرر ادرار و همچنين تغييراتي در رگهاي خوني بدن ( سرخرگها و سياهرگها) ميشود. ديابت ميتواند به اشكال مختلف روي ديد تاثير بگذارد. باعث ايجاد آب مرواريد ، آب سياه و مهمتر از همه صدمه به رگهاي خوني داخل چشم ميشود.
Diabetic retinopathy is an eye condition that can cause vision loss and blindness in people who have diabetes. It affects blood vessels in the retina (the light-sensitive layer of tissue in the back of your eye). If you have diabetes, it's important to get a comprehensive dilated eye exam at least once a year. Diabetes can lead to swelling in the macula, which is called diabetic macular edema. Over time, this disease can destroy the sharp vision in this part of the eye, leading to partial vision loss or blindness. Macular edema usually develops in people who already have other signs of diabetic retinopathy.
Who is more likely to develop diabetic eye disease?
Anyone with diabetes can develop diabetic eye disease. Your risk is greater with
high blood glucose that is not treated
high blood pressure that is not treated
High blood cholesterol and smoking may also raise your risk for diabetic eye disease.
Some groups are affected more than others. African Americans, American Indians and Alaska Natives, Hispanics/Latinos, Pacific Islanders, and older adults are at greater risk of losing vision or going blind from diabetes.
If you have diabetes and become pregnant, you can develop eye problems very quickly during your pregnancy. If you already have some diabetic retinopathy, it can get worse during pregnancy. Changes that help your body support a growing baby may put stress on the blood vessels in your eyes. Your health care team will suggest regular eye exams during pregnancy to catch and treat problems early and protect your vision.
Diabetes that occurs only during pregnancy, called gestational diabetes, does not usually cause eye problems. Researchers aren't sure why this is the case.
Your chances of developing diabetic eye disease increase the longer you have diabetes.
رتينوپاتي ديابتي چيست؟
رتينوپاتي ديابتي عارضه اي ناشي از ديابت است كه بدليل تغييرات ايجاد شده در رگ هاي خوني رخ مي دهد. پرده شبكيه لايه عصبي در پشت چشم است كه نور را درك ميكند و تصاوير را به مغز ميفرستد. وقتي عروق خوني در شبكيه آسيب ميبينند ممكن است باعث نشت مايع يا خون شده يا منجر به رشد شاخههاي عروقي شكننده و كلافه مانند شده و باعث تخريب شبكيه شود در نتيجه تصويري كه شبكيه به مغز ميفرستد تار شده يا كج و معوج ميشود.
رتينوپاتي ديابتي يكي از علل اصلي كاهش ديد است و كسانيكه ديابت درمان نشده دارند 25 برابر شانس بيشتري براي كوري نسبت به افراد عادي دارند.
هرچه طول بيماري ديابت بيشتر باشد احتمال رتينوپاتي ديابتي بيشتر ميشود. در نزديك به 80% كسانيكه لااقل 15 سال ديابت دارند مقداري صدمه به عروق شبكيه ديده ميشود. در مبتلايان به ديابت نوع يك (نوع جوانان ) احتمال ابتلا به رتينوپاتي ديابتي در سنين پايين تر بيشتر است. چنانچه شما ديابت داريد بايستي بدانيد كه امروزه با بهبود وسائل تشخيصي و درماني، فقط درصد كوچكي از بيماران مبتلا به ديابت مشكلات جدي ناشي از كاهش ديد خواهند داشت، مشروط به اينكه به موقع به چشم پزشك مراجعه نمايند.
انواع رتينوپاتي
Diabetes Type
Duration of Disease
Probability of Retinopathy
Probability of Progression
Type I
10 years
60 to 74%
Unspecified
Type I
15 years
98%
25% proliferative retinopathy
Type I
20 years
100%
50% proliferative retinopathy
Type II
At diagnosis
10 to 20%
Unspecified
Type II
4 years
4 to 29%
Unspecified
Type II
15 years
60 to 80%
5 to 20% proliferative retinopathy
Table1. Incidence of retinopathy relative to duration of Type I and Type II diabetes http://lieyecare.com/diabetic.html
رتينوپاتي زمينه اي مرحله اول رتينو پاتي ديابتي است. در اين مرحله عروق كوچك در پرده شبكيه صدمه ديدهو مايع يا خون از آنها نشت ميكند. مايع نشت كرده باعث تورم پرده شبكيه شده و يا رسوباتي بنام "اگزودا" را ايجاد مينمايد.
با اينكه اين مرحله معمولاً روي ديد تاثيري نميگذارد اما ممكن است بعداً به مراحل شديدتري كه منجر به كاهش ديد ميشود تبديل شود. از اين رو رتينوپاتي زمينه اي به عنوان يك علامت هشداردهنده محسوب ميشود.
گاهي مايعي كه نشت كرده است در مركز ديد جمع ميشود. مركز ديد مسئول ديدن جزئيات ريز اشيا ميباشد (مثلاً حروف يا اعداد). اين مسئله بنام تورم مركز ديد خوانده ميشود و ممكن است سبب شود خواندن يا انجام كارهاي نزديك مشكلتر شود.
رتينوپاتي پروليفراتيو(تكثيري) حالتي است كه رگهاي خوني جديد و غيرطبيعي بروي سطح شبكيه رشد ميكنند. اين پديده "نئوواسكولاريزاسيون - Neovascularization" خوانده مي شود. اين عروق جديد ديواره ضعيفتري داشته و شكننده هستند و ممكن است منجر به خونريزي شوند. زجاجيه ماده شفاف و ژله مانندي است كه مركز چشم را پر ميكند. خون نشت كرده باعث كدر شدن زجاجيه شده و بصورت نسبي عبور نور را از مردمك به پرده شبكيه را مانع ميشود در نتيجه تصوير تار و درهم ميشود . اين رگهاي خوني غيرطبيعي ممكن است تبديل به بافت سفتي شده كه شبكيه را از پشت چشم جدا كنند و باعث جدا شدگي پرده شبكيه شوند كه در صورت عدم درمان ميتواند منجر به كاهش شديد ديد و كوري شود.
رگهاي خوني غيرطبيعي همچنين ممكن است اطراف مردمك ، روي عنبيه (قسمت رنگي چشم) رشد كرده و با افزايش فشار داخل چشم باعث ايجاد آب سياه شود.
رتينوپاتي ديابتي تكثيري (پروليفراتيو) شديدترين نوع بيماري شبكيه ناشي از ديابت ميباشد. حدود 20% افراد ديابتي به آن مبتلا ميشوند و ميتواند باعث كاهش شديد ديد و كوري شود.
معمولاً در مرحله رتينوپاتي زمينه اي علامتي وجود ندارد. اگرچه ممكن است در صورت ايجاد تورم مركز ديد تاري ديد بصورت تدريجي ايجاد شود. شما ممكن است هرگز به تغيير ميزان ديد خود پي نبريد. معاينه چشم پزشكي تنها راهيست كه به كمك آن ميتوان تغييرات داخل چشم شما را پيدا كرد.
وقتيكه خونريزي ايجاد ميشود ديد شما تار شده، لكههايي در آن پيدا ميشود و حتي ممكن است بكلي ديد شما از بين برود. رتينوپاتي ديابتي پروليفراتيو اگرچه بدون درد است اما شكل شديدي از بيماري است و نيازمند توجه پزشكي فوري است.حاملگي و افزايش فشار خون ممكن است رتينوپاتي ديابتي را تشديد كنند.
چگونه رتينوپاتي ديابتي تشخيص داده ميشود؟
بهترين راه براي تشخيص رتينوپاتي ديابتي معاينه چشمي در فواصل منظم ميباشد كه توسط چشم پزشك بايستي انجام شود. رتينوپاتي بسيار شديد ممكن است كاملاً بدون علامت باشد. بيماري را ميتوان با درمان بهبود بخشيد. براي تشخيص رتينوپاتي ديابتي چشم پزشك با استفاده از دستگاهي بنام افتالموسكوپ بداخل چشم شما نگاه ميكند. چشم پزشكي ممكن است قبل از معاينه با استفاده از قطره چشمي مردمك را باز كند.
چنانچه چشم پزشك رتينوپاتي ديابتي را تشخيص دهد ممكن است نياز به عكس رنگي ته چشم يا آزمايش خاصي بنام "آنژيوگرافي با فلوئورسئين" باشد تا مشخص شود كه شما احتياج به درمان داريد يا نه؟ در آنژيوگرافي با فلوئورسئين يك ماده رنگي به داخل رگ شما تزريق ميشود و عكسهاي مخصوصي از چشم شما گرفته ميشود.
چگونه رتينوپاتي ديابتي درمان ميشود؟
براي درمان چشم پزشك مسائل زير را در نظر ميگيرد:
سن شما
تاريخچه پزشكي شما
چگونگي نحوه زندگي شما
چه مقدار شبكيه صدمه ديده است ؟
در بسياري موارد احتياجي به درمان نيست اما بيمار بايد بطور مرتب تحت معاينات چشمي قرار گيرد. در ديگر موارد، درمان براي متوقف كردن صدمات ناشي از رتينوپاتي ديابتي و در صورت امكان بهبود ديد انجام ميشود.
كرايوتراپي(سرد كردن): اگر زجاجيه بدليل وجود خون كدر باشد جراحي ليزر را تا زمانيكه خون جذب شود نميتوان انجام داد. در بعضي موارد خونريزي زجاجيه، كرايوتراپي يا يخ زدن شبكيه ممكن است در كوچك شدن رگهاي خوني غيرطبيعي كمك كننده باشد.
ويتركتيومي (برداشتن زجاجيه): در رتينوپاتي ديابتي پروليفراتيو پيشرفته ممكن است چشم پزشك برداشتن زجاجيه را توصيه كند. اين جراحي ميكروسكوپي در اطاق عمل انجام ميشود. ويتركتيومي زجاجيه پر شده از خون را بر مي دارد و به جاي آن ماده شفافي را جايگزين ميكند. در حدود 70% بيماران بعد از برداشتن زجاجيه بهبودي ديد دارند . گاهي اوقات قبل از انجام عمل برداشتن زجاجيه چشم پزشك ممكن است براي چند ماه يا يكسال صبر كند تا شايد خونريزي خود بخود جذب شود.
ترميم شبكيه: در صورتيكه بافت تخريب شده منجر به جداشدگي شبكيه از پشت چشم شود كاهش شديد ديد يا كوري را باعث ميشود مگر اينكه جراحي براي چسباندن شبكيه بموقع و با موفقيت انجام شود.
نقش بيمار در درمان چيست ؟
مراقبت موفقيت آميز رتينوپاتي ديابتي فقط به درمان اوليه توسط چشم پزشك شما بستگي ندارد. طرز برخورد و توجه شما به درمان داروئي و رعايت رژيم ديابتي ضروري است. شما بايستي ميزان مناسب قند خون خود را حفظ كنيد. از سيگار كشيدن خودداري كنيد و به فشار خون خود نيز توجه داشته باشيد. فعاليتهاي فيزيكي معمولاً براي بيماران مبتلا به رتينوپاتي ديابتي مسئله اي نيست . گاهي در بيماران مبتلا به نوع فعال رتينوپاتي پروليفراتيو محدود كردن فعاليتهاي فيزيكي توصيه ميشود.
كاهش ديد به ميزان زيادي قابل پيشگيري است
رتينوپاتي ديابتي ممكن است بدون هيچ گونه علامتي وجود داشته باشد.
تشخيص اوليه رتينوپاتي ديابتي بهترين روش براي جلوگيري از كاهش ديد است.
بيماران مبتلا به ديابت بايستي حداقل سالي يكبار توسط چشم پزشك معاينه شوند. وقتيكه رتينوپاتي ديابتي ايجاد شد معاينات بيشتر چشم پزشكي با فواصل كمتر ضروري است.
با كنترل دقيق چشم پزشك ميتوانيد درمان را قبل از صدمه ديد شروع كنيد.
The first step in a contact lens fitting is a consideration of your lifestyle and your preferences regarding contact lenses, such as whether you might want to change your eye color with color contact lenses or if you're interested in options such as daily disposables or overnight wear. Although most people choose soft contact lenses, the advantages and disadvantages of rigid gas permeable (GP) lenses will likely be discussed as well.
If you are over age 40 and need bifocals, your eye doctor or contact lens specialist will discuss ways to deal with this need, including multifocal contact lenses and monovision (a prescribing technique where one contact lens corrects your distance vision and the other lens corrects your near vision). Contact lens measurements Just as one shoe size doesn't fit all feet, one contact lens size doesn't fit all eyes. If the curvature of a contact lens is too flat or too steep for your eye's shape, you may experience discomfort or even damage to your eye. Measurements that will be taken to determine the best contact lens size and design for your eyes include:
Corneal curvature: An instrument called a keratometer is used to measure the curvature of your eye's clear front surface (cornea). This measurement helps your doctor select the best curve and diameter for your contact lenses. If your eye's surface is found to be somewhat irregular because of astigmatism, you may require a special lens design of lens known as a "toric" contact lens. At one time, only gas permeable contact lenses could correct for astigmatism. But there are now many brands of soft toric lenses, which are available in disposable, multifocal, extended wear and colored versions.
In some cases, a detailed mapping of the surface of your cornea (called corneal topography) may be done. Corneal topography provides extremely precise details about surface characteristics of the cornea and creates a surface "map" of your eye, with different contours represented by varying colors.
Pupil and iris size: The size of your pupil and iris (the colored part of your eye) can play an important role in determining the best contact lens design, especially if you are interested in GP contact lenses. These measurements may be taken with a lighted instrument called a biomicroscope (also called a slit lamp) or simply with a hand-held ruler or template card.
Tear film evaluation: To be successful wearing contact lenses, you must have an adequate tear film to keep the lenses and your cornea sufficiently moist and hydrated. This test may be performed with a liquid dye placed on your eye so your tears can be seen with a slit lamp, or with a small paper strip placed under your lower lid to see how well your tears moisten the paper. If you have dry eyes, contact lenses may not be right for you. Also, the amount of tears you produce may determine which contact lens material will work best for you.
The optic nerve contains axons of nerve cells that emerge from the retina, leave the eye at the optic disc, and go to the visual cortex where input from the eye is processed into vision. There are 1.2 million optic nerve fibers that derive from the retinal ganglion cells of the inner retina.
Optic neuropathy refers to damage to the optic nerve due to any cause. Damage and death of these nerve cells, or neurons, leads to characteristic features of optic neuropathy. The main symptom is loss of vision, with colors appearing subtly washed out in the affected eye. On medical examination, the optic nerve head can be visualised by an ophthalmoscope. A pale disc is characteristic of long-standing optic neuropathy. In many cases, only one eye is affected and patients may not be aware of the loss of color vision until the doctor asks them to cover the healthy eye. eResearch by Navid Ajamin -- summer 2012
Optic neuropathy is often called optic atrophy, to describe the loss of some or most of the fibers of the optic nerve. In medicine, "atrophy" usually means "shrunken but capable of regrowth", so some argue that "optic atrophy" as a pathological term is somewhat misleading, and the term "optic neuropathy" should be used instead.
In short, optic atrophy is the end result of any disease that damages nerve cells any where between the retinal ganglion cells to the lateral geniculate body(anterior visual system).
What causes optic neuropathy?
What Causes Optic Neuritis?
Infections such as toxoplasmosis.
Ocular herpes.
Other viral infections.
Sinusitis.
Neurological disorders.
Leber hereditary optic neuropathy, an inherited form of vision loss that affects mostly males in their 20s or 30s.
Nutritional deficiency.
Toxins, including alcohol and tobacco.
Reference:
Optic neuropathy
Optic neuritis and neuropathy: Symptoms, causes, treatments
See Also: Optic nerve atrophyU.S. National Library of Medicine
Age-related macular degeneration (AMD) is a medical condition which usually affects older adults and results in a loss of vision in the center of the visual field (the macula) because of damage to the retina. It occurs in “dry” and “wet” forms. It is a major cause of blindness and visual impairment in older adults (>50 years). Macular degeneration can make it difficult or impossible to read or recognize faces, although enough peripheral vision remains to allow other activities of daily life.[1]
Age-related macular degeneration (AMD) is an eye disease that can blur your central vision. It happens when aging causes damage to the macula — the part of the eye that controls sharp, straight-ahead vision. The macula is part of the retina (the light-sensitive tissue at the back of the eye).[9]
Dry macular degeneration, also known as atrophic or non-neovascular age-related macular degeneration (AMD), is a common eye condition that primarily affects the macula, the central part of the retina responsible for sharp, central vision. In dry AMD, there is a gradual breakdown or atrophy of the light-sensitive cells in the macula, particularly the retinal pigment epithelium (RPE) cells. These cells are crucial for supporting the health and function of the photoreceptor cells, including cones, in the macula.
The condition progresses slowly over time and can lead to symptoms such as blurred central vision, distorted vision (metamorphopsia), and difficulty seeing in low light. Unlike wet AMD, which involves abnormal blood vessel growth, dry AMD typically does not involve leaking blood vessels.
There are two main types of dry macular degeneration:
Early and Intermediate Dry Macular Degeneration: In the early stages, small yellow deposits known as drusen may form beneath the retina. Drusen are accumulations of waste materials that can interfere with the normal functioning of the macula. At this stage, individuals may not experience significant vision loss, and the condition may be detected during a routine eye exam.
Advanced Dry Macular Degeneration (Geographic Atrophy): Over time, some individuals with dry AMD may progress to an advanced stage characterized by the development of geographic atrophy. Geographic atrophy involves the loss of RPE cells and photoreceptor cells in discrete patches, leading to the formation of atrophic or “geographic” areas in the macula. This can result in a more significant and irreversible loss of central vision.[8]
Macular Degeneration - Symptoms and Detection Symptoms of Dry AMD include the presence of drusens that begin to enlarge. Another symptom is blurry areas in central vision. A symptom of Wet AMD is seeing straight lines as wavy ones.
A visual acuity test can help an eye care professional determine if any central vision is lost. An Amsler grid may also be used to detect AMD. In this test you cover one eye and stare at a black dot that has patterns of straight lines. If these lines appear wavy or are missing then AMD could be present.[2]
Prevention
There is growing evidence that by improving your diet, you may also improve the health of your eyes. Research has suggested an association between macular degeneration and a high saturated fat diet.
There is also evidence that eating fresh fruits and dark green, leafy vegetables – foods rich in vitamins C and E, selenium, and carotenoids (including beta-carotene, lutein and zeaxanthin) – may delay or reduce the severity of AMD.
How AMD can affect your sight?
AMD is progressive and it is also painless. While AMD may affect your central vision, most people still retain useful side (or peripheral) vision. Key symptoms of AMD include:
Distortion, where straight lines may appear wavy or bent. For example, lines of tiles in the bathroom appear wavy.
Difficulty in reading or doing any other activity which requires fine vision.
Difficulty in distinguishing faces.
Dark patches or empty spaces, which appear in the centre of your vision.
The need for increased illumination, sensitivity to glare, decreased night vision and poor colour sensitivity.[6]
Foods to Enjoy eResearch by Navid Ajamin -- spring 2012
Eat the freshest and brightest fruits and vegetables. Pick the most colorful vegetables and fruits you can find - red, dark green, orange, or yellow. These foods play a key role in keeping your eyes healthy:
Carrots Corn Kiwi Pumpkin Yellow squash Zucchini squash Red grapesGreen peas Cucumber Butternut squash Green bell pepper Celery Cantaloupe Sweet potatoes Dried apricots Tomato and tomato products Dark green leafy vegetables SpinachKaleTurnips Collard greens ...
Fish
Eating fatty fish such as salmon, tuna or mackerel two to three times per week can slow the progression of age-related macular degeneration (AMD) according to a study published in the British Journal of Ophthalmology.
This research further confirms earlier studies that suggested eating fish can help reduce the risk of getting AMD and demonstrates that some of those already affected by the disease can benefit as well.
Nuts
Nuts not only contain Omega-3 fatty acids, but also copper which can play a role in preventing age-related eye diseases. Even just a handful of nuts at two or three times a week can reduce your risk of AMD.
Foods to Avoid
A high-fat, high-cholesterol diet can lead to fatty plaque deposits in the macular vessels, which can hamper blood flow and increase the risk of AMD. A diet low in fat promotes good eye health. Skip foods and processed baked goods with high-fat content. In addition recent research has indicated that those consuming red meat (10 times a week or more) were at 47% higher risk for macular degeneration.
Vitamins and Supplements
The National Eye Institute’s Age-Related Eye Disease Study (AREDS) found that taking a specific high-dose formulation of antioxidants and zinc significantly reduces the risk of advanced AMD and its associated vision loss. Slowing AMD’s progression from the intermediate stage to the advanced stage will save the vision of many people.
People who should consider taking the combination of antioxidants plus zinc include those who are at high risk for developing advanced AMD. These people are defined as having either:
Intermediate AMD in one or both eyes. Intermediate AMD is defined as the presence of either many medium-sized drusen or one or more large drusen.
Advanced AMD in one eye, but not the other eye. Advanced AMD is defined as either a breakdown of light-sensitive cells and supporting tissue in the central retinal area (advanced dry form), or the development of abnormal and fragile blood vessels under the retina (wet form) that can leak fluid or bleed. Either of these forms of advanced AMD can cause vision loss. Ask you doctor if taking this special formulation is right for you and where you can obtain the specific formula in your country.[3]
Grapes May Help Prevent AMD
Can eating grapes slow or help prevent the onset of age-related macular degeneration (AMD), a debilitating condition affecting millions of elderly people worldwide? Results from a new study published in Free Radical Biology and Medicine suggest this might be the case. The antioxidant actions of grapes are believed to be responsible for these protective effects.[4]
Home Remedies and Lifestyle Changes [7]
The risk factors for macular degeneration are similar to those of heart disease and stroke.For this reason, lifestyle changes that benefit your heart may also benefit your vision. Lifestyle modifications to consider include:
Quitting smoking
Making dietary changes, such as limiting foods high in saturated fats (meat, butter, and cheese) and eating a heart-healthy diet full of whole grains, fruits, and vegetables
Maintaining weight, since obesity is also a risk factor of dry AMD
Managing blood pressure
Using sun protection, such as wearing wide-brimmed hats and sunglasses
Getting regular exercise (at least 30 minutes of physical activity every day)
As central vision declines in late-stage dry AMD, you can use low-vision tools, such as magnifying tools and handheld computers, to help with daily activities. Low-vision techniques, like using high-lumen light sources, reducing glare, and increasing contrast, can also help compensate for central vision loss.
Discussion. This systematic review and meta-analysis has shown that 8·7% of the worldwide population has age-related macular degeneration, and the projected number of people with the disease is around 196 million in 2020, increasing to 288 million in 2040.[5]
Different Types of Glaucoma There are several different categories of glaucoma which include: Open Angle Glaucoma, Narrow Angle Glaucoma, Congenital Glaucoma and Secondary Glaucoma. [1]
Types of glaucoma[2]
There are four main types of glaucoma:
primary open angle glaucoma
primary angle closure glaucoma
secondary glaucoma
developmental glaucoma
Open Angle Glaucoma Open Angle Glaucoma is the most common form of glaucoma and is a result of the trabecular meshwork becoming less efficient over time. In this case, the eye continues to produce the same amount of aqueous humor, but the trabecular meshwork is not able to keep up. This imbalance of fluid production and drainage results in an excess amount of aqueous fluid. As the fluid builds up, the intraocular pressure (IOP) elevates. As a consequence to this elevation in eye pressure, the optic nerve becomes damaged.
For most people with open angle glaucoma, there are no perceivable symptoms in the early stages of the disease. However, as the optic nerve is continually subjected to an environment of increased eye pressure, it becomes damaged. This damage is eventually perceived as peripheral visual field defects. If the eye pressure is not monitored or controlled, open angle glaucoma can eventually lead to blindness. eResearch by Navid Ajamin -- autumn 2011
An ideal intraocular pressure is different for each individual. Some patients are able to tolerate a higher eye pressure while others cannot. It is important to be followed regularly by your eye doctor to determine an appropriate target IOP and ensure that this pressure is maintained over time.
Symptoms of glaucoma often do not show up until considerable visual loss has occurred. This is not the case for diabetics, however. Someone with diabetes is at much higher risk for vision loss.
Narrow Angle Glaucoma Narrow Angle Glaucoma is less common than Open Angle Glaucoma. People who are farsighted (hyperopic) are more susceptible to this form of glaucoma because they typically have smaller eyes, although Narrow Angle Glaucoma can occur in nearsighted eyes. A smaller eye correlates to more crowding of the structures within the eye. In a normal eye there is sufficient space between the iris (the colored part of the eye) and the trabecular meshwork. However, in a crowded eye, the space between the iris and the trabecular meshwork is narrowed.
The iris controls the amount of light that enters the eye. Under bright light conditions the iris contracts to cover more space and make the pupil smaller (minimizing the amount of light that enters the eye). In dark lighting conditions, the iris dilates to allow more light to enter the eye. In a person with narrow angles, as the pupil dilates the iris can completely block the trabecular meshwork drainage angle. This can result in a rapid rise in eye pressure and can lead to an angle closure glaucoma attack.
An individual suffering from an angle closure attack typically experiences a severe headache above the eye brow, eye pain, significant eye redness, the pupil becomes fixed and dilated, the vision is significantly blurred, halos are seen around lights and nausea and vomiting can occur. An angle closure glaucoma attack is an emergency and must be treated immediately. Unfortunately, the damage done to the optic nerve during an angle closure glaucoma attack can be significant and is permanent. In some cases, Angle Closure Glaucoma can present insidiously however, without sudden symptoms.
Preventing Angle Closure Fortunately, there is a means of preventing angle closure attacks. Narrow angles can be diagnosed during a routine eye exam. At that time, the doctor will look at the trabecular meshwork drainage angle through a special contact lens. This testing, referred to as gonioscopy, allows the doctor to determine the degree of narrowing. If the angles are very narrow, the doctor may recommend a laser procedure known as Laser Peripheral Iridotomy. During this in-office (out-patient) procedure, a small hole is created in the iris. This microscopic hole allows for another route for the aqueous fluid to enter the anterior chamber, and allows the iris to fall away from the drainage angle. The doctor makes the hole on the top part of the iris that is usually covered by the eyelid.
As with any surgical procedure, there are some risks to Laser Peripheral Iridotomy. However, the risks of the procedure are minimal and if the procedure is recommended, the benefit of the procedure in reducing the risk of angle closure glaucoma outweighs the risk of the procedure. Some of the risks include blurred vision, slight bleeding or inflammation within the eye. Some people notice a twinkle or flicker of light or shadow image after the procedure. These symptoms can arise from the affect of light entering the small hole in the iris. This side effect of the procedure is very unusual; in most cases, the upper eyelid covers the location of the iridotomy and the optical side effect is not perceived. Occasionally, the procedure needs to be repeated if the iridotomy heals over.
Imaging the angle. A slice through the front of two eyes taken with a special camera shows an open angle above and a closed angle below (images made with anterior segment optical coherence tomography). The arrow points to where the iris is separate from the cornea in the open angle (upper picture). In the lower picture, the iris is so close to the cornea that it nearly touches the trabecular meshwork (in front of arrowhead).[3]
Congenital Glaucoma Congenital Glaucoma is a result of the malformation of the trabecular meshwork drainage angle during fetal development. The defective trabecular meshwork impedes the proper drainage of the aqueous fluid within the eye causing an increase in intraocular pressure. The elevated eye pressure eventually leads to damage of the optic nerve, which may result in blindness. For this reason it is imperative that children afflicted by the disease be seen by an ophthalmologist regularly in hopes of preserving as much of the child’s vision as possible.
Congenital glaucoma is generally diagnosed within the first few months of a child’s life. Infants with congenital glaucoma often have symptoms of tearing, red eye, light sensitivity and a cloudy appearance of the eye. In the far majority of congenital glaucoma cases, both eyes are affected by the disease. Males are more commonly afflicted with this disease than females; however, congenital glaucoma is rare, affecting approximately 0.05% of children.
Secondary Glaucoma Secondary glaucoma is an acquired form of glaucoma and may present itself as open angle or angle closure glaucoma. This type of glaucoma can be a result of trauma, inflammatory diseases, tumors or use of corticosteroids. Secondary glaucoma may be temporary.
Traumatic Secondary Glaucoma In the circumstance of either blunt or penetrating ocular trauma, the trabecular meshwork can be damaged. This damage leads to the trabecular meshwork inefficiently draining the aqueous fluid out of the eye. As a result, the amount of aqueous fluid in the eye builds and increases the intraocular pressure. This increase in eye pressure leads to damage of the optic nerve. Eventually, the optic nerve damage results in visual field defects, and in some cases blindness.
Inflammatory Glaucoma and Steroid Responders Inflammatory diseases such as uveitis can also lead to secondary glaucoma. Additionally, most cases of uveitis are treated with corticosteroids. Unfortunately, one of the side effects of corticosteroid use can be a significant increase in intraocular pressure. This cyclic condition is often a tight-rope-walk for the ophthalmologist to effectively treat the ocular inflammation while trying to maintain an adequate intraocular pressure.
Pseudoexfoliative Glaucoma One of the more common forms of secondary glaucoma is referred to as pseudoexfoliation glaucoma. This type of secondary glaucoma occurs when the eye forms material that can affect the drainage angle. Like a clogged sink, the fluid is unable to properly drain and fluid accumulates within the eye. This accumulation of fluid can lead to an increase in eye pressure and eventually damage the optic nerve.
Pigmentary Glaucoma Similarly, pigmentary glaucoma is another form of secondary glaucoma. Pigmentary glaucoma is a result of the iris pigment breaking off. These pigment granules can then clog the drainage angle and induce glaucoma.
Neovascular Glaucoma Neovascular glaucoma is another form of secondary glaucoma. This form of glaucoma typically affects individuals with diabetes, or eyes that have circulation problems in the retina or in the arteries that supply the eye. Neovascularization refers to the new growth of abnormal blood vessels. The new blood vessels can block the trabecular meshwork and lead to high eye pressure. This form of glaucoma can be difficult to treat.
ICE Syndrome ICE is an acronym for, “IridoCorneal Endothelial” syndrome. This is a very rare form of glaucoma that typically affects one eye. The condition occurs when the endothelial layer (the most inner layer) of the cornea grows over the trabecular meshwork and across the surface of the iris. This causes an increase in intraocular pressure and leads to damage of the optic nerve. These abnormal endothelial cells form adhesions that attach the iris to the cornea, which in turn blocks the drainage angle further.[1]
What we see is the result of signals sent from the eyes to the brain. Usually the brain receives signals from both (bi) eyes (ocular) at the same time. The information contained in the signal from each eye is slightly different and with well-functioning binocular vision, the brain is able to use these differences to judge distances and coordinate eye movements.
Binocular vision anomalies are among the most common visual disorders. They are usually associated with symptoms such as headaches, eye strain, eye pain, blurred vision, and occasionally double vision. There are many reasons binocular vision might become reduced or lost altogether, including: Reduced vision in one eye, Loss of coordination of movement between the two eyes (strabismus) and Problems with the brain comparing images from both eyes.[12]
In Binocular Vision Dysfunction(BVD), the line of sight from one eye tends to be slightly out of alignment with the line of sight from the other eye. This misalignment can be vertical, horizontal or both and puts heavy strain on the eye muscles as they are constantly trying to correct the misalignment to achieve single focus. This heavy strain on the eye muscles results in dizziness, headaches, disorientation, neck aches and reading difficulties. These common symptoms are not traditionally thought to be to be associated with your vision but they are.
Symptoms of Binocular Dysfunction may include: (the inability to coordinate the eyes together effectively)
Only being able to read for short periods
Difficulty maintaining body control
Bumping into walls or objects
Occasionally seeing double
Poor depth perception
Frequent eye rubbing
Poor handwriting
Motion sickness
Double vision
Visual fatigue
Headaches
Who should receive a Binocular Vision Assessment?
The short answer is that anyone with two eyes has the potential to need a Binocular Vision Assessment.
The main groups of people that we see for Binocular Vision Assessments include:
Amblyopia – Amblyopia, sometimes called lazy eye, is a vision condition where one or both eyes fails to see 20/20 because of barriers to visual development. Amblyopia often results in glasses wear and patching, but should also include a Binocular Vision Assessment. If one eye is weaker than the other, an assessment of eye teaming should be performed so further treatment can be initiated. Treatment prescribed at a Binocular Vision Assessment helps many patients with amblyopia achieve 20/20 vision even when their previous doctor told them nothing more could be done.
Strabismus – This is a general term for eye turn. An eye turn is a form of binocular vision dysfunction (makes sense right, the eyes have such a hard time working together that one turns away). There are several treatment options for strabismus and a Binocular Vision Assessment allows the doctor to determine the best treatment course for the specific case.
Double Vision – Double vision results when the two eyes do not work together. People who see double, even occasionally, should have a Binocular Vision Assessment to determine
1) what is causing the double vision 2) how to resolve the double vision.
Headaches – Not every headache is caused by vision. But if you get headaches after reading, working on the computer, or at the end of a school or work day it is important to rule out vision as a contributing factor.
Eyestrain – This one seems obvious, and an eye exam with the right doctor can solve many cases of eyestrain. Many doctors, however, do not test the necessary visual skills that result in eyestrain, which is why a Binocular Vision Assessment is needed.
Struggling Students – 80% or more of what we learn in class occurs through the visual system. This creates a situation where many struggling students have undiagnosed vision conditions (1 in 4 students actually have a vision condition significant enough to impact learning). Step number one with a struggling student: make sure they can see and hear. This means more than can they see 20/20 and can they hear the tone. A Binocular Vision Assessment evaluates the visual skills necessary for success in the classroom.
Acquired Brain Injury Patients – Head injuries result in a number of visual deficits, often times affecting the visual skills evaluated in a Binocular Vision Assessment. A Neuro-Optometric Assessment, performed by an optometrist with residency-training in neuro-optometry, is tailored to the needs of acquired brain injury patients. Rehabilitation cannot be successful if visual barriers are not addressed early in the process. You must see to improve.
Patients in Occupational, Speech or Balance Therapy – Vision plays a central role with most everything we do. If a person is receiving therapy for deficits in one area, vision should be evaluated prior to therapy to know if additional visual barriers are present. Handwriting is a visual-motor task. Language requires sight-sound connections. Balance relies of visual-vestibular input.
Athletes – Competitive sports require extremely high levels of visual function. An Athlete Vision Assessment is tailored to the needs of athletes and the specific visual demands of their sport.
Along with the aforementioned symptoms of BVD, additional problems associated with the condition include:
Vertical Heterophoria (VH). This is a condition in which there’s a very slight, often imperceptible difference in the height of the eyes. The right eye may be marginally higher than the left eye or vice versa. If not detected and treated, VH can cause pain and discomfort throughout the patient’s life.
Post Concussive Syndrome. This condition can develop following a blow to the head sustained during a sporting event, motor vehicle accident, military action or other trauma. When a patient has post concussive syndrome, the headaches and dizziness that commonly characterize the condition can last for weeks or even months.
There are three forms of Binocular Vision Dysfunction:
Vertical heterophoria
Superior oblique palsy
horizontal misalignment
Vision Therapy
Vertical heterophoria can be present at birth, but symptoms can only occur later in life after prolonged strain on the muscles surrounding the eye. The eyes will try to overcompensate for the small height difference and move up or down straining the eye muscles continuously so images can be seen clearly together, instead of resulting in double vision. However, after a certain time, prolonged eye muscle strain can lead to vertical heterophoria. The muscles simply give out. This is when symptoms of dizziness, headaches, and blurred vision appear.[10]
Superior oblique palsy is an eye disorder involving a weak or paralyzed superior oblique muscle, responsible for rotation. It can be congenital, or acquired through an injury.[9]
Sensory strabismus is strabismus due to vision loss or impairment, leading to horizontal, vertical or torsional misalignment or to a combination thereof, with the eye with poorer vision drifting slightly over time. Most often, the outcome is horizontal misalignment.[11]
The corrective measures taken by the eye muscles in order to keep the lines of sight aligned, i.e. vision that is not blurred or double, results in overuse of the eye muscles making them strained and fatigued which results in many of the symptoms of BVD. Head tilt is known to occur in Vertical Heterophoria and Superior Oblique Palsy to minimize misalignment and avoid double vision. In order to achieve single focused vision, the brain takes a corrective measure by tilting the head slightly resulting in neck pain and other BVD symptoms.[8]
Our visual system has evolved to keep track of head and body movements
Most people get along just fine without true binocular vision. Some do have some difficulty with certain tasks under certain situations. Driving a motor vehicle, especially if the left eye is blurred or otherwise unused, can sometimes be troublesome. Threading a needle is chore. Some sports need good binocular vision as does viewing holographs.
A young child who is delayed in learning to walk or, later, bumps into things (more than normal) should be examined by an eye doctor, preferably an optometrist or someone who understands and can test binocular function. Sometimes there is a fairly straightforward diagnosis and management plan. There are a number of vision system causes for loss of binocular function. It is possible, although much more rare, for higher level neurological dysfunction to be the culprit. These would be problems within the brain or the connections between the eyes and the visual processing center in the brain. eResearch by Navid Ajamin -- Spring 2011
What are the causes for loss of binocular vision? There are number of causes for the lose of binocular vision. The two primary issues are amblyopia and strabismus.[1]
What Is a Binocular Vision Assessment
What is Binocular Vision? Usually the brain gets images from both (bi) eyes (ocular) at the same time. The brain combines the two images into one, to make vision. The images that the brain gets from the eyes are however slightly different from each other. The brain uses these small differences to work out how far away an object is. This is called depth perception. It can also help to work out how quickly an object is moving towards or away from a person. This is a type of movement perception.
What causesloss of binocular vision? There are lots of reasons why binocular vision might become reduced or lost altogether.
Reasons include:
Reduced vision in one eye
Loss of coordination of movement between the two eyes (squint)
Problems with the brain comparing images from both eyes [2]
Binocular Vision Problems Headaches, eyestrain, fatigue, blurred and double vision are common symptoms for someone with a binocular vision problem. A perfectly healthy eye with 20/20 vision can still have a disorder of the focusing system or the extra-ocular muscles. Binocular vision problems can be a major problem for young students and can impact reading and learning.
Vision therapy can effectively treat and relieve the symptoms of most binocular vision problems. All children should have a professional eye exam before 30 months, to rule out any possible binocular vision problems.[3]
Why Binocular Vision Dysfunction in Children Is Frequently Mistaken for Something Else
Binocular interaction Apart from binocular summation, the two eyes can influence each other in at least three ways.
Pupillary diameter. Light falling in one eye affects the diameter of the pupils in both eyes. One can easily see this by looking at a friend's eye while he or she closes the other: when the other eye is open, the pupil of the first eye is small; when the other eye is closed, the pupil of the first eye is large.
Accommodation and vergence. Accommodation is the state of focus of the eye. If one eye is open and the other closed, and one focuses on something close, the accommodation of the closed eye will become the same as that of the open eye. Moreover, the closed eye will tend to converge to point at the object. Accommodation and convergence are linked by a reflex, so that one evokes the other.
Interocular transfer. The state of adaptation of one eye can have a small effect on the state of light adaptation of the other. After effects induced through one eye can be measured through the other.[4]
With stereo vision you see an object as solid in three spatial dimensions--width, height and depth--or x, y and z. It is the added perception of the depth dimension that makes stereo vision so rich and special.
Stereopsis (from the Greek στερεο- stereo- meaning "solid", and ὄψις opsis, "appearance, sight") is a term that is most often used to refer to the perception of depth and 3-dimensional structure obtained on the basis of visual information deriving from two eyes by individuals with normally developed binocular vision. Because the eyes of humans, and many animals, are located at different lateral positions on the head, binocular vision results in two slightly different images projected to the retinas of the eyes. The differences are mainly in the relative horizontal position of objects in the two images. These positional differences are referred to as horizontal disparities or, more generally, binocular disparities. Disparities are processed in the visual cortex of the brain to yield depth perception. While binocular disparities are naturally present when viewing a real 3-dimensional scene with two eyes, they can also be simulated by artificially presenting two different images separately to each eye using a method called stereoscopy. The perception of depth in such cases is also referred to as "stereoscopic depth".[7]
There are two aspects of stereopsis: the nature of the stimulus information specifying stereopsis, and the nature of the brain processes responsible for registering that information.
The distance between the two eyes on an adult is almost always 6.5 cm and that is the same distance in shift of an image when viewing with only one eye. Retinal disparity is the separation between objects as seen by the left eye and the right eye and helps to provide depth perception. Retinal disparity provides relative depth between two objects, but not exact or absolute depth. The closer objects are to each other, the retinal disparity will be small. If the objects are farther away from each other, then the retinal disparity will be larger. When objects are at equal distances, the two eyes view the objects as the same and there is zero disparity.[4]
Retinal disparity, sometimes called binocular disparity, is part of the process in visual perception that generates the depth and dimensionality. In the sequence of perception, this would occur at the surface/object stage. Specifically, retinal disparity is the space between the eyes that allows binocular vision to create depth perception.
The diagram below indicates a left and right eye. Both eyes converge on a box but due to retinal disparity, the angle of viewing is slightly different for each eye. The brain combines the two images to create the perception of a three-dimensional object.[13]
Retinal disparity is usually thought of as a 2D vector representing the deviation from retinal correspondence. It's assumed to decompose naturally into two orthogonal components, called horizontal and vertical disparity. Extensive literature has shown these components to be processed in fundamentally different ways. But when eye movements and non-identical correspondence patterns are taken into account, the simple definition of retinal disparity breaks down. In general, neither horizontal, nor vertical disparity, nor, indeed, the disparity vector itself, are well defined entities. Retinally, a binocular target is represented by one 2D position vector for each eye, or four dimensions. If disparity is assumed to be the difference between these projection vectors and a retinal correspondence pattern, the resulting entity has eight degrees of freedom - four more than a retinally located 2D disparity vector would have. Only when empirical retinal correspondence obeys certain constraints can disparity be reduced to such a vector. But even then it can not be simply split into retinal horizontal and vertical components, because moving eyes change the relationship between retinal locations and epipolar projection geometry. A practical consequence of these theoretical issues is demonstrated using the induced effect as an example.[14]
Stereoscopy creates the illusion of three-dimensional depth from given two-dimensional images. Human vision, including the perception of depth, is a complex process, which only begins with the acquisition of visual information taken in through the eyes; much processing ensues within the brain, as it strives to make sense of the raw information. One of the functions that occur within the brain as it interprets what the eyes see is assessing the relative distances of objects from the viewer, and the depth dimension of those objects.[6]
Stereo Vision Has Many Advantages
Stereo vision--or stereoscopic vision --probably evolved as a means of survival. With stereo vision, we can see WHERE objects are in relation to our own bodies with much greater precision--especially when those objects are moving toward or away from us in the depth dimension. We can see a little bit around solid objects without moving our heads and we can even perceive and measure "empty" space with our eyes and brains.[5]
Two Eyes = Three Dimensions (3D) Each eye captures its own view and the two separate images are sent on to the brain for processing. When the two images arrive simultaneously in the back of the brain, they are united into one picture. The mind combines the two images by matching up the similarities and adding in the small differences. The small differences between the two images add up to a big difference in the final picture! The combined image is more than the sum of its parts. It is a three-dimensional stereo picture.[5]
Stereoblindness (also stereo blindness) is the inability to see in 3D using stereopsis, or stereo vision, resulting in an inability to perceive stereoscopic depth by combining and comparing images from the two eyes.
WHAT IS A CATARACT (CAT-ah-rackt)? The word cataract is derived from a Greek word meaning "waterfall" (looking through falling water). Cataracts are most commonly caused by chemical changes within the lens of the eye, which is thought to be part of the natural aging process.[1]
A cataractis a gradual clouding of the eye's natural lens. The formation of a cataract occurs during the normal process of aging. Although cataracts may affect people of any age, they are most common in older adults. Because cataracts form gradually, the symptoms are often difficult to spot. Perhaps you have noticed increased difficulty when driving toward the sun, find it harder to see traffic lights against a bright sky, or find it takes longer for your vision to return to normal after passing an oncoming set of bright headlights.
Symptoms include reduced depth perception, diminished color perception, annoying glare in sunlight, and poor night vision. Headaches, eye fatigue, burning, and watering of the eyes when exposed to bright light are also some other symptoms attributed to cataracts.[2]
More than half of all Americans age 65 and older have cataracts.
What Causes Cataracts?
The eye functions much like a camera. Light rays enter the eye, passing through the cornea, the aqueous humor -- transparent fluid in the front of the eye -- and then the pupil and into the lens. The lens bends the light rays to focus objects onto the retina lining the back of the eye. From there, the image passes through the retinal cells, into the optic nerve, and finally to the back of the brain which process the images.
Cataracts occurwhen there is a buildup of protein in the lens that makes it cloudy. This prevents light from passing clearly through a the lens, causing some loss of vision. Since new lens cells form on the outside of the lens, all the older cells are compacted into the center of the lens resulting in the cataract.
Types of cataracts include:
Age-related cataracts. As the name suggests, this type of cataract develops as a result of aging.
Congenital cataracts. Babies are sometimes born with cataracts as a result of an infection, injury, or poor development before they were born, or they may develop during childhood.
Secondarycataracts. These develop as a result of other medical conditions, like diabetes, or exposure to toxic substances, certain drugs (such as corticosteroids or diuretics), ultraviolet light, or radiation.
Traumatic cataracts. These form after injury to the eye.
Other factors that can increase a person's risk of developing cataracts include cigarette smoke, air pollution, and heavy alcohol consumption.
What Are the Symptoms of Cataracts?
Cataracts usually form slowly and cause few symptoms until they noticeable block light. When symptoms are present, they can include:
Vision that is cloudy, blurry, foggy, or filmy.
Progressive nearsightedness in older people often called "second sight" because they may no longer need glasses.
Changes in the way you see color because the discolored lens acts as a filter.
Problems driving at night such as glare from oncoming headlights.
Diplopiais the medical term for double vision.It is caused due to defective functioning of the extraocular muscles or a disorder of the nerves that stimulate the muscles. Usually, double vision is a symptom of strabismus, i.e.,squint.
Strabismus is a misalignment or deviation of the two eyes. All types of strabismus do not give rise to double vision.A person suffering from diplopia loses his ability to walk, read, and do routine activities.
Diplopia caused by other conditions[3]
Diplopia is often caused by other issues and conditions in your body and eyes. That’s why it’s so important to get your eyes checked right away when you notice any changes in your vision.
Diplopia and myasthenia gravis
People with myasthenia gravis have muscle weakness that worsens throughout the day. This can affect your ocular muscles (the muscles that control your eyes and eyelids) and cause double vision.
Diplopia and proptosis
Proptosis is the bulging of one or both of your eyes from their natural position. Bulging eyes are usually caused by thyroid issues, like Graves' disease or hyperthyroidism, and may come with diplopia.
Diplopia and keratoconus
Keratoconus occurs when your cornea (the clear part of your eye that you see through) loses its shape. Usually, your corneas are round, but keratoconus causes your cornea to bulge outward like a cone. This distorted shape causes vision issues, including diplopia.
Diplopia and vertigo
Vertigo is a sensation that the environment around you is spinning in circles. It’s usually caused by issues in your inner ear. However, if you’re experiencing severe double vision, you might feel vertigo, too. Diplopia and vertigo are usually symptoms of other issues in your body.
Diplopia and diabetes
If you have diabetes, your body isn’t able to properly process and use glucose from the food you eat. Diabetes can damage your eyes and cause symptoms like diplopia and serious issues like diabetes-related retinopathy.
What are the symptoms of diplopia?
Other than seeing double, diplopia can be associated with other symptoms like:
Headache.
Nausea (upset stomach or feeling sick).
Dizziness.
Pain (including when you move your eyes).
Blurred or unclear vision in one or both eyes.
The brain of a young child with strabismus (paralytic, congenital, or accommodative) tends to suppress the unwanted second image produced by misaligned strabismic eye so that only one image is seen by the child. This natural attempt of the body to prevent double vision leads to poor vision in the affected eye. The only symptom observed in diplopia is the visualization of two images of the same object.
Usually, there is paralysis of one or more of the eye muscles in diplopia. So, movement of the eye in a particular condition is not possible. Double vision can be overcome by tilting or turning the head. Image separation can occur temporarily due to a growth in the eyelid pressing upon the front of the eye ball. The eyeballs themselves may protrude (exophthalmos) as a result of overfunctioning of the thyroid gland (hyperthyroidism). Swelling and scarring within the eyelid can also produce double vision. In rare cases, an eye abnormality can cause diplopia. For example, a dislocated lens will result in the passing of light rays only partly through itself with the rest spreading over the surrounding area. This leads to the formation of two images on the retina. eResearch by Navid Ajamin -- spring 2011
The management of diplopia may entail the use of prisms(optical devices used to deviate images),orthoptics (treatment by exercises to strengthen the eye muscles), occlusion (covering the abnormal eye), and eye muscle surgery. these may be tried out alone or in various combinations, the basic goal being to restore binocular vision, where the person sees only a single image. The cause of strabismus should be ascertained early in the case of children, so that corrective treatment can be started immediately. In adults, double vision needs to be treated urgently to avoid the progression of a probable tumor, aneurysm, or neurological abnormality. If the diplopia is a result of some severe underlying pathology, the cause should be treated first. Surgical intervention should always be the last resort.
Diplopia refers to the simultaneous perception of two images of a single object that may be displaced horizontally or vertically in relation to each other. It is also called double vision. The condition can affect balance, movement, and reading ability.
Physiological and pathological
It is of two types – (1)Physiological, (2)Pathological
Physiological Diplopia Or “normal double vision” is a phenomenon where objects are doubled, either in front of Or behind, whatever target you are focusing on. Usually, it doesn’t impinge on consciousness.
Pathological Diplopia divided into two types (a)Binocular Diplopia, (b) Uniocular/ Monocular Diplopia. [5]
Diplopia may be preventable in certain cases. For example, post-traumatic double vision can be avoided by wearing a seat belt when driving a four-wheeler and a helmet when riding a two-wheeler. This will reduce the impact of the injury. While indulging in any sports activity, it is advisable to wear protective headgear and glares to protect the head and the eyes respectively. Similarly, if your occupation exposes you to the risk of suffering an eye injury, special precautions must be taken. If you are a diabetic, you should ensure that you maintain your blood sugar levels close to normal in order to avoid diplopia caused by nerve damage.[1]
In this disease, the victim observes double image of anything. Following are the kinds of this disease-
1.Binocular diplopia: In it, an object is observed by both eyesseparately.
2.Vertical diplopia: In this kind of diplopia, one image appears above the other in the same vertical plane.
3.Monocular diplopia or unocular diplopia: In it, double vision of one image is seen.
4.Dierect diplopia, homonimus diplopia: Double visionin which right-hand image appears on the right side and left-hand image on the left-side.
5.Crossed diplopmia, heteronymous diplopia: Double vision in which right-hand image appears on the left-side and left-hand image on the right-side.[2]
What tests will be done to diagnose this condition?
If you have monocular diplopia, you likely won’t need additional tests beyond having your eyes examined. If you have binocular diplopia, you might need imaging tests, including:
Magnetic resonance imaging (MRI).
CT (computed tomography) scan.
Blood tests.
These tests will capture a complete picture of your eyes and the area around them. They’ll help your provider identify issues with your bones, brain or spine.
How can I prevent diplopia?
There aren’t any ways to specifically prevent experiencing double vision, but taking good care of your eyes and seeing your healthcare provider regularly are the best ways to catch issues before they cause you pain or other symptoms. Follow these steps to maintain good eye health:
Don’t smoke.
Give your eyes a break from looking at electronic screens throughout the day.
Wear appropriate protective glasses or goggles for all of your work, sports or other activities.
Schedule an eye exam every one to two years (or as often as your healthcare provider recommends).
The Potential Causes of Double Vision in Kids
What causes ghosting vision or double vision?
There are actually a variety of different things that can cause diplopia. First, it should be made clear that there is a difference between long-term and short-term diplopia. Long-term diplopia is a lengthier health issue which can be an indication of major health issues. In contrast, short-term diplopia is usually not a serious concern for your long-term health since the causes of it are easily overcome. As a matter of fact, many of us have suffered from double vision temporarily before. Short-term double vision is often caused by temporary and more easily combated factors such extreme fatigue, extensive alcohol or drug consumption. [4]
Long-term or recurring diplopia, however, can be caused by many different issues in the body.
Some of these issues can actually become life-threatening conditions.
1) Corneal irregularities – The cornea is the transparent layer on the outer edge of your eye that helps focus images onto your retina so you can see clearly. Any irregularity with this clear outer edge could certainly cause long-term ghosting or double vision.
2) Severely dry eyes– If your eyes don’t produce sufficient tears, they will also have a hard time focusing and operating optimally. Conditions that cause dry eyes, such as Sjogren’s syndrome, can often cause sufferers to have double or ghosting vision as well.
3) Cataracts– Since the lens part of your eye becomes cloudy when a cataract develops and because cataracts don’t attack both eyes simultaneously, they are a common cause of ghosting vision in one eye.
4) Cranial nerve palsies – A cranial nerve palsy happens when one or more of the muscles that control the eyes and its ability to focus get paralyzed or can’t coordinate any longer with the other muscles that control the eye. This cause of double vision can be caused by a variety of things such as head injuries, multiple sclerosis, diabetes, tumors, a blockage of an artery and other serious health conditions.
5) Brain tumor, stroke or a brain aneurysm – These type of illnesses and conditions are usually extremely serious and can even be life-threatening. Since these conditions can happen out of the blue, so do the corresponding diplopia symptoms that can come with them. This is why it is extremely important to see a doctor if you are ever suffering from double vision and don’t know what its cause is.
Glaucoma is a multi-factorial, complex eye disease with specific characteristics such as optic nerve damage and visual field loss. While increased pressure inside the eye (called intraocular pressure or IOP) is usually present, even patients with normal range IOP can develop glaucoma.
There is no specific level of elevated eye pressure that definitely leads to glaucoma; conversely, there is no lower level of IOP that will absolutely eliminate a person’s risk of developing glaucoma. That is why early diagnosis and treatment of glaucoma is the key to preventing vision loss.
Eye pressure is measured in millimeters of mercury (mm Hg). Normal eye pressure ranges from 12-22 mm Hg, and eye pressure of greater than 22 mm Hg is considered higher than normal. When the IOP is higher than normal but the person does not show signs of glaucoma, this is referred to as ocular hypertension.
High eye pressure alone does not cause glaucoma. However, it is a significant risk factor. Individuals diagnosed with high eye pressure should have regular comprehensive eye examinations by an eyecare professional to check for signs of the onset of glaucoma.
In the past, eye care professionals sometimes referred to a person with an elevated IOP as a glaucoma suspect, because of the concern that the elevated eye pressure might lead to glaucoma. However, the term glaucomasuspect is usually reserved today to describe a person who has suspicious optic nerve cupping in the setting of normal IOP and normal visual fields.
In the majority of cases, vision loss usually occurs when the eye pressure is too high for the specific individual and damages the optic nerve. Any resultant damage cannot be reversed. In eyes with glaucoma, peripheral (side) vision is affected first. The changes in vision may be so gradual that they are not noticed until a lot of vision loss has already occurred.
In time, if the glaucoma is not treated, central vision will also be decreased and then lost — this is how blindness from glaucoma is most often noticed. The good news is that glaucoma can be managed if detected early, and with medical and/or surgical treatment, most people with glaucoma will not lose their sight.
If you are at higher risk for glaucoma, you should have a thorough eye exam every one or two yearsafter age 35. If you are diagnosed with glaucoma, it is important to work with your eye doctor and carefully follow your prescribed treatment. Glaucoma medications will only work if they are taken exactly as advised by your doctor, so it is important to follow your medication regimen carefully.
شايد بتوان گفت بينائى مهمترين حس انسان است. نه تنها به اين علت که در ارتباط با محيط خارج از بدن، نقش مهمى دارد، بلکه از اينرو که اختلال ديد، سبب کاهش يادگيرى نيز مىشود. شخص با حس بينائى مىتواند از خود محافظت کند، تعادل خود را نگهدارد، خلاقيت داشته باشد و بالاخره از ديدن محيط اطراف لذت ببرد. لذا از چشمها بايد نهايت مواظبت بهعمل آمده و براى بهداشت آن به نکات زير توجه گردد:
هرگز نبايد دست آلوده را به چشم ماليد. دست و صورت خصوصاً دستها بايد مرتب با آب و صابون شسته شود. از شستن دست و صورت در آبهاى آلوده و کثيف، جداً بايد خوددارى گردد.
بايد از حوله و دستمال شخصى و تميز استفاده کرد و هرگز حوله و دستمال ديگران را مورد استفاده قرار نداد.
مطالعه بايستى در نور کافى انجام گيرد و از خواندن نوشتههاى خيلىريز خوددارى شود.
بههنگام مسافرت با اتومبيل و ساير وسايط نقليه، حتىالمقدور از مطالعه خوددارى شود.
فاصله چشم از کتاب بايد حدود ۳۰ سانتىمتر و زاويه کتاب نسبت به سطح مورد مطالعه ۴۵ تا ۷۰ درجه باشد.
از خيرهشدن به نور شديد، مانند خورشيد و لامپهاى پرنور خوددارى شود. همچنين در مقابل آفتاب، باد، گرد و خاک، از چشمها محافظت شود.
براى خواب و استراحت، اتاق بايد تاريک باشد تا اعصاب چشم بهخوبى استراحت کند.
مصرف غذاهاى داراى ويتامين A و پروتئين در حفظ سلامت چشم اهميت بهسزائى دارد.
اختلالات بينائى در سلامت دانشآموز و پيشرفت تحصيلى او اثر زيادى دارد و بايد مورد توجه مسئولان آموزشگاه قرار گيرد. آموزگار، مدير، پزشک، مربى بهداشت در تأمين سلامت بينائى شاگردان مسئوليت مشترک دارند. آموزگار بهعلت تماس دائمى با شاگردان، بهتر از هر شخص ديگر با توجه دقيق، به خواندن و نوشتن و کار کردن آنها مىتواند افرادى را که داراى اختلال يا ضعفى در قوه بينائى هستند، بشناسد و پس از آزمايش، آنها را نزد پزشک هدايت نمايد.
بهطور کلى علائمى که شخص با ديدن آن علائم، بايد متوجه اختلالاتى در دستگاه بينائى خود گردد، عبارتند از:
- اگر اشياء و نوشتهها را در فاصله معمولى بهخوبى نتوان مشاهده نمود و يا هنگام نگاهکردن به آنها احساس ناراحتى کرد.
- اگر در هنگام غروب آفتاب نتوان بهخوبى ديد.
- اگر احساس شود که چشم زود خسته مىشود.
- اگر گاهى سردرد، بهخصوص هنگام غروب عارض شود.
- اگر چشم، خارش و سوزش داشته باشد و يا درد بگيرد.
- اگر صبحها، هنگام بيدار شدن، در گوشه چشم ترشحاتى جمع شود.
با مشاهده علائم بالا، لازم است به چشم پزشک مراجعه نموده و دستورات وى را به دقت بهکار برید.
اختلالات بينائى
دوربينى، نزديکبينى، و آستيگماتيسم، از اختلالات عمده بينائى در دانشآموزان به شمار مىرود. دوربينى در افراد دوربين، اشعههاى نورانى که بهطور موازى به چشم مىتابد، در عقب شبکيه، تشکيل تصوير مىدهد که اين اختلال گاهى علل ارثى دارد. دانشآموزانى که به اين عارضه دچار هستند، چشمان خود را زياد مىمالند. در موقع کارهاى ظريف مضطرب و بىقرار هستند. در موقع خواندن يا نوشتن، سر را دورتر از حد معمول نگاه مىدارند. به خواندن يا ديدن کتابهاى مصور تمايلى نشان نمىدهند. درد چشم، سردرد، التهاب پلک، تيک صورت و گاهى سرگيجه دارند. براى درمان دوربيني، از عينکهاى با عدسى محدب استفاده مىگردد.
نزديکبينى در افراد نزديکبين، اشعه نورانى که به چشم مىتابد جلوتر از شبکيه، تشکيل تصوير مىدهد. نزديکبينى به حالت و عادت کسانى که چشم خود را تنگ مىکنند تا بهتر ببينند، اطلاق مىشود. فاکتورهائى نظير کار نزديک، کمى نور، کمبود ويتامينها و غيره در ايجاد نزديکبينى مؤثر هستند. دانشآموزانى که به اين عارضه دچارند، اغلب موقع نگاهکردن به دور، گردن مىکشند. در موقع نوشتن يا خواندن، سر را از حد معمول نزديکتر مىبرند. گاهى يک چشم را مىبندند و با تنگ نمودن چشم ديگر، سعى در تطابق اجسام دارند. سردرد و آبريزى از چشم نيز مشاهده مىگردد. براى درمان نزديکبيني، از عينکهاى با عدسى مقعر مناسب استفاده مىگردد.
آستيگماتيسم اين عارضه از عيوب انکسارى چشم است. در اين عارضه، تصوير يک نقطه همان يک نقطه درک نمىشود، بلکه از يک نقطه از هر جسم خارجي، دو خط افقى ديده مىشود. در اين حالت بعضى از اشعههاى نوراني، يکديگر را روى شبکيه قطع مىکنند، در حالىکه محل تلاقى پارهاى ديگر، در جلو يا عقب شبکيه است و تصويرى که ايجاد مىکند، زياد روشن و واضح بهنظر نمىرسند. دانشآموزان مبتلا به آستيگماتيسم، اغلب سر را به کتاب يا تصوير نزديک مىکنند، سردرد دارند و چشم را هنگام مشاهده تصاوير ظريف مىمالند. تصحيح چشم آستيگمات اغلب ساده بوده و با استفاده از عدسى استوانهائى که در جهت مناسبى از چشم قرار داده مىشود، انجام مىگيرد. مگر در بعضى حالات نادر که تصحيح آن بسيار مشکل بوده و گاهى حتى غيرممکن است.
Cataracts are a common age-related vision problem. About 20.5 million Americans age 40 and older have cataracts, and the older a person gets the greater the risk for developing cataracts. Women are more likely to develop cataracts than men, and African Americans and Hispanic Americans are at particularly high risk.
Congenital cataracts: Causes, types and treatment
In addition to age, other factors may increase the risk of cataract development.
These include: Diabetes، Smoking، Over-exposure to sunlight
Symptoms
During the early stages, cataracts may have little effect on vision. Symptoms vary due to the location of the cataract in the eye (nuclear, cortical, or posterior subcapsular). Depending on the type and extent of the cataract, patients may experience the following symptoms:
- Cloudy vision
- Double or blurry vision
- Glare and sensitivity to bright lights
- Colors appear faded
- Difficulty reading due to reduced black-white contrast[2]
- Sudden nearsightedness
- Changes in the way you see color, especially yellow
- Problems driving at night because oncoming headlights are distracting
- Problems with glare
- Sudden temporary improvement in close-up vision
Types of cataracts include: eResearch by Navid Ajamin -- winter 2010
Age-related cataracts. As the name suggests, this type of cataract develops as a result of aging.
Congenital cataracts. Babies are sometimes born with cataracts as a result of an infection they had before they were born, or they may develop during childhood.
Secondary cataracts. These may develop as a result of other diseases, like diabetes, or long-term exposure to toxic substances, certain medications (such as corticosteroids or diuretics), ultraviolet light, and radiation.
Traumatic cataracts. These can form after injury to the eye.
A cataract can be congenital (a person is born with it) or can be acquired or developmental (it appears later in childhood or in adulthood).
Common causes include:
heredity (inheriting a cataract from a parent)
trauma (injury) to the eye
radiation (treatment for cancer)
medication (for example steroids)
other illnesses or conditions (for example Down syndrome)
infection (for example German measles).
In many cases, however, the cause of a cataract is not known.
Cataracts do not go away by themselves, except in a few rare situations.
Mild cataract
If the cataract is small and does not affect your child's vision, the doctor may decide not to treat it at all or may prescribe special eye drops to dilate (widen) the pupil to allow more light to enter the eye. If your child needs eye drops, make sure you carefully follow the instructions for putting them in.
Serious cataract
If the cataract is more serious, your child will need surgery to remove it. Cataracts cannot be removed with medication or lasers.
? What Causes Cataracts
Key points
A cataract is a cloudy area over the lens of the eye. In children under nine, it stops the eye's vision from developing normally and can cause amblyopia.
If the cataract is mild, the doctor may decide to prescribe eye drops to make the pupil bigger or not to treat it at all if the vision is not affected. If the cataract is serious, the only way to treat it is to remove all or some of the lens during surgery.
After surgery, your child will need a corrective device such as a contact lens, intra-ocular lens or, in rare situations, eye glasses. Your child will also need to wear a patch to help both eyes develop equally strong vision.
Your eye doctor will need to check your child's vision regularly after surgery. It is extremely important that you keep all follow-up appointments.
Please call the eye doctor if your child has increased pain, swelling or sensitivity to light after surgery or if their corrective device causes any redness, swelling, discharge, pain or other unusual symptoms.[3]
Other cataract types include:
Pediatric cataracts. Pediatric cataracts affect babies and children. Babies may be born with cataracts (congenital), or the cataracts may form sometime after birth. Pediatric cataracts typically run in families, but they can also happen due to eye injuries or other eye conditions. Babies and children with pediatric cataracts need prompt treatment to prevent problems like amblyopia (lazy eye).
Traumatic cataracts. These cataracts form when something injures your eye. Treatment for this type is more complicated because structures around the lens may also need repair.
Secondary cataracts. These are cloudy patches that form on your lens capsule, or the membrane that covers your lens. Another term for this condition is posterior capsular opacification. It’s a common but easily treatable complication of cataract surgery.
Understanding early-onset cataracts
Types of age-related cataracts
There are several types of age-related cataracts. Their names refer to their location in your lens. To understand these types, it helps to learn a bit about the anatomy of your lens.
Your lens is made up of a few layers. You can think of them like the layers of an apple:
The nucleus is in the center of your lens. It’s like the core of the apple.
The cortex is the layer that surrounds the nucleus. It’s like the fruit you eat that surrounds the core.
The lens capsule is the thin membrane covering the cortex. It’s technically not part of the lens itself, but is instead like a close-fitting skin that covers and protects the lens. The lens capsule is a bit like the apple skin.
Eye care providers classify cataracts based on where they form in your lens. Often, people have more than one type at the same time. That’s because it’s common for cloudy patches to form in multiple areas of your lens. The three most common types of age-related cataracts are:
Nuclear sclerotic cataract, which forms in the nucleus.
Cortical cataract, which forms in the cortex.
Posterior subcapsular cataract, which forms in the posterior cortex. “Posterior” in this context means the “back” of your lens. This is the part that’s closest to your retina (which is behind your lens). “Subcapsular” means the cataract forms at the outer edge of the cortex, just beneath the lens capsule.
myths about childhood cataracts
What can be mistaken for cataracts?
Glaucoma and cataracts are both common degenerative eye conditions and potential causes of blindness. Both conditions can be age related and eventually lead to reduction in sight, which is why they often get confused.[13]
Is cataract genetic?
Cataracts can be hereditary, as parents may pass down genetic mutations that cause the disease. However, most cases of cataracts are due to the cumulative effects of lifelong environmental exposures and aging. Cataract surgery is an effective and safe treatment for the condition.[12]
What common disease affects the lens?
Cataracts. Refractive errors like astigmatism, farsightedness (hyperopia), nearsightedness (myopia), and age-related loss of up-close focusing (presbyopia). Glaucoma. Age-related macular degeneration.[11]
What causes cataracts in pregnancy? Disease factors suffered by the mother such as low blood sugar, lack of oxygen, and hypothermia. Infectious factors in the body attack pregnant women such as chickenpox, influenza, and polio as well as metabolic disorders.[8]
Causes of acquired cataracts [7]
Cataracts that develop in children after they're born are known as acquired, infantile or juvenile cataracts.
Causes of this type of cataracts can include:
Why cataracts develop in young people
galactosaemia – where the sugar galactose (which mainly comes from lactose, the sugar in milk) cannot be broken down by the body
diabetes – a lifelong condition that causes a person's blood sugar level to become too high
eye trauma – as a result of an injury to the eye or eye surgery
toxocariasis – a rare parasitic infection that can sometimes infect the eyes, spread from animals to humans via their infected faeces
But most of these problems are either rare or do not usually cause cataracts to develop in children.
At what age do cataracts usually start?
The proteins in your eye’s lens start to break down around age 40. But you typically won’t notice symptoms until age 60 or later. Certain medical conditions, like diabetes, may cause you to have symptoms sooner.
How common are cataracts?
Cataracts are very common in the U.S. and globally. According to the World Health Organization, about 17% of people around the world have cataracts that cause problems with their vision. However, the prevalence varies widely by country and region. There’s a higher prevalence in middle-income and low-income nations where people often have more risk factors and limited access to cataract treatment.
In the U.S., nearly 1 in 5 people age 65 to 74 have cataracts that affect their vision. More than 50% of people over age 80 either have cataracts or had surgery to remove them.[4]
What deficiency causes cataracts?
?Does screen time lead to pediatric cataracts
Vitamin B2 and vitamin B3 are needed to protect glutathione, an important antioxidant in the eye. Vitamin B2 deficiency has been linked to cataracts. Older people taking 3 mg of vitamin B2 and 40 mg of vitamin B3 per day were partly protected against cataracts in one trial.[5]
What increases the risk of cataracts?
Family history of cataracts at a young age. Years of excessive exposure to the sun and UV rays. Smoking. Obesity.[6]
What is the most common cause of congenital cataracts?
Genes and genetic conditions
Recent research suggests genetic causes are responsible for the majority of bilateral congenital cataracts in the UK. Cataracts can also be associated with conditions caused by chromosome abnormalities, such as Down's syndrome.[7]
What systemic diseases cause cataracts?
Alcohol intake and nutritional status may play a role in cataract formation. Cataract has been associated with many systemic diseases mainly diabetes mellitus, hypertension, obesity, chronic kidney disease and autoimmune disease. Cataract is also a hallmark of many metabolic disorders and syndromes.[9]
What are the biochemical causes of cataract?
Conclusions: Hyperglycemia, hypernatremia, hypokalemia and hypocalcemia can independently increase the patients' risk to cataracts. Corrections in these biochemical parameters may reduce cataract incidence.[10]
In the normal eye, light rays pass through the cornea, pupil, and lens and focus directly on the retina. When the cornea fails to focus light rays directly on the retina, refractive errors such as myopia, hyperopia, and astigmatism occur.
What should a normal eye look like?
The white part of the eye, the sclera, with the overlying conjunctiva, is not red and inflamed. The cornea is bright and clear. The pupil is black and round. If the pupil and iris are well seen, this confirms that the cornea must be clear.
Myopia
Myopia, or nearsightedness, occurs when the curvature of the cornea is too steep or the eyeball is too long. Therefore, light rays entering the eye focus in front of the retina. This results in blurred vision at distance.
Hyperopia
Hyperopia, or farsightedness, occurs when the curvature of the cornea is too flat or the eyeball is too short. Therefore, light rays entering the eye focus in back of the retina. This results in blurred vision at near.
Astigmatism
Astigmatism occurs when the curvature of the cornea is irregularly shaped, like the shape of a football. Therefore, light rays entering the eye focus at two different foci, causing blurred or distorted vision at distance and near. Astigmatism can occur alone or in conjunction with myopia and hyperopia.
Presbyopia
Presbyopia is a vision condition in which the crystalline lens loses its flexibility or elasticity, making it difficult to focus on near objects. Generally, presbyopia becomes noticeable in the early to mid-40s. Presbyopia is an unpreventable age-related process. To help alleviate symptoms of presbyopia, reading glasses, bifocals, progressive lenses, and multifocal contact lenses can be prescribed.
Dry Eye Syndrome
Dry eye syndrome is a physical condition in which the front of the eye becomes dry. Symptoms of dry eyes will affect the majority of people at some time. Patients with dry eyes often report feelings of sandy, gritty, burning, tearing, and itchiness in the eye. Other symptoms include fluctuation in vision, contact lens intolerance and recurrent infections. Symptoms may worsen in hot and dry climates and can become more irritated by smoke, wind, and air conditioned environments.
Achieving relief from the symptoms of dry eye is easy with dry eye therapy. Therapy may be as simple as using over the counter artificial tears, but may be complex to involve the use of prescription medications and/or punctal plugs. A dry eye therapy plan is covered by most major medical insurances and can be easily implemented to help relieve the pesky ailments of dry eyes.
What is thyroid eye disease?
Also known as TED (thyroid eye disease) or Graves’ eye disease, thyroid eye disease is an autoimmune disorder involving an imbalance or recognition problem with your immune system.
Most commonly, this happens as part of thyroid disease from an overactive thyroid gland, affecting the skin and eyes. This autoimmune disease causes inflammation and swelling, stimulating the production of muscle tissue and fat behind the eye. Up to one-half of people with Graves’ disease develop these eye symptoms.
Stages of thyroid eye disease
There are two phases of thyroid eye disease. The first is the inflammatory phase which can last from six months to two years, while the second is the stable phase, during which the active inflammation is dormant.
Following the inflammatory phase, many individuals are left with eye protrusion, eyelid retraction, or double vision, which can be treated in various ways. If you believe you have thyroid eye disease, you must talk to your doctor immediately.
What does thyroid eye disease look like?
Thyroid eye disease symptoms can vary significantly from one person to another. For some individuals, symptoms can lead to pain, disfigurement, or threatened eyesight. For others, the disorder remains unchanged for many years but for others it can either worsen or slightly improve.
Allergy and Infections
Red eyes that itch and burn are commonly related to an allergy or in worse cases, an infection. Allergies are common and often present symptoms similar to those of dry eyes, but will definitely become more prevalent during hay fever season. Irritations caused by allergies can be alleviated with prescription eye drops.
When allergy-like symptoms are accompanied with pain or discomfort, eye secretions, vision loss, and light sensitivity, it may be due to an eye infection. Infections of the eyes may result from many scenarios, such as eye abrasions from injuries, foreign bodies, or contact lens wear. Symptoms of an emerging infection can be easily dismissed for an allergy or dry eye, hence it is important that all patients seek immediate care for any suspicious redness, pain, or sudden loss of vision.
Cataract
Cataract is the clouding of the eye’s natural crystalline lens. This loss of transparency decreases the amount of light that can reach the retina, resulting in overall blurriness of images. Signs and symptoms of cataract include: blurry, hazy vision, reduced intensity of colors, increased sensitivity to glare, increased difficulty with night vision, and changes in the eye’s refractive error. Cataracts are typically due to age-related changes in the natural lens. Other precipitating factors may include: ultraviolet radiation exposure, diabetes, corticosteroid use, smoking, high alcohol consumption, and certain nutrient deficiency. Recent studies have shown that antioxidants (e.g. vitamin C, vitamin E, carotenoids) may decrease cataract formation.
Glaucoma
Glaucoma is an eye disease caused by an increased pressure in the eye. This can damage the optic nerve that transmits visual information to the brain, resulting in the loss of vision. Glaucoma is the second leading cause of blindness in the U.S. Individuals over the age of 40, individuals with a family history of glaucoma, and African Americans are at an increased risk of developing glaucoma. Other risk factors for the development of glaucoma include: thinner corneas, systemic vascular conditions (e.g. diabetes, hypertension, heart disease), prolong corticosteriod use, high myopia, chronic ocular inflammation, and ocular trauma.
What is Retinal Vein Occlusion?
Retinal Vein Occlusion (RVO) is a condition where the veins carrying blood away from the retina, located at the back of the eye, become blocked. This blockage causes blood and fluid to leak into the retina, leading to visual problems.
Macular Degeneration
Macular degeneration (MD) is the leading cause of blindness in Americans over the age of 55. MD causes a deterioration and loss of photoreceptors and other cells in the macula, the part of the retina responsible for sharp, clear central vision. Because only central vision is usually affected, people rarely go blind from the disease. However, MD can sometimes make it difficult to read, drive, or perform other daily activities that require fine, central vision. Most people with MD have the dry form, for which there is no known treatment. The less common wet form may respond to laser procedures, if diagnosed and treated early. A major National Eye Institute study (AREDS) indicates that certain nutrients such as beta carotene (vitamin A) and vitamins C and E may help prevent or slow progression of MD. eResearch by Navid Ajamin -- winter 2010
Retinal Detachment
The retina is the light-sensitive tissue that lines the inside back wall of the eye. In retinal detachment, the retina is separated from its underlying supportive tissue, depriving it from nutrients and oxygen. The longer the retina is detached, the greater the risk of permanent vision loss. Retinal detachment, thus, is a medical emergency requiring prompt surgical treatment to preserve vision. Warning signs of retinal detachment include: floaters, flashes of light, a sudden decrease in vision, and a shadow or curtain over the vision. Risk factors for retinal detachment include: high myopia, previous severe eye injury/trauma, family history of retinal detachment, and previous history of retinal detachment in the other eye.
Unusual Eye Conditions You Didn’t Know About
3Meter (10ft) HOTV Translucent Eye Chart
In any medical field, there are always going to be certain medical conditions that we see on a daily basis. For ophthalmologists, common conditions include glaucoma, which per the Glaucoma Research Foundation afflicts over 3 million people, and cataracts, which according to the National Eye Institute, half of individuals will have a cataract or cataract surgery by the age of 80. However, there are also eye-related medical conditions that people may never encounter. The following rare eye conditions appear in less than .01% of United States citizens, per the National Eye Institute.
Anophthalmia and Microphthalmia
While these two rare eye conditions are commonly used in substitution for each other, they are actually two separate but related conditions. Anophthalmia is a birth defect that results in the absence of one or both eyes. Micropthalmia is when one or both eyes is noticeably too small.
In the cases of both conditions, genetic mutations and abnormal chromosomes are believed to be at fault. Environmental factors are a challenge to pinpoint, put researchers have suggested X-rays, chemicals, drugs, pesticides, toxins, radiation and viruses may also be to blame. In other words, more research is still needed to determine what causes this defects.
Bietti’s Crystalline Dystrophy
Back in 1937, Italian ophthalmologist Dr. G. B. Bietti had three different patients with similar symptoms. Crystals were in the cornea and yellow shiny deposits were on the retina. Eventually, the back layers of the eye – the retina, choriocapillaries and choroid – would begin to atrophy. In patients since, crystals have also been found in white blood cells.
Currently, there is no treatment for BCD, though some believe that treatment will arise out of more genetic research.
Retinitis Pigmentosa
Retinitis Pigmentosa refers to a group of rare genetic disorders, all of which lead to the breaking down of cells in the retina. The retina is responsible for processing light and hosts rods and cones that interpret color and allow us to see at night. In RP, over 50 different genes can be afflicted. When the genetic mutations are severe enough, the cells in the retina aren’t provided with enough protein to function. In some cases, the protein is toxic. Over time, RP will cause the rods and cones in the eyes to die, impeding night and peripheral vision. Patients with the condition will also often find bright lights uncomfortable. Treatments for Retinitis Pigmentosa includes low-vision improvement aids for children and vitamin A drops for adults.
Retinoblastoma
Perhaps the most life-threatening and most rare eye condition on the list, retinoblastoma is a cancer that affects the retina. Unfortunately, it is most commonly found in children under the age of five. The good news is that if the cancer is diagnosed early enough and treatment is delivered promptly, the vision and life of the child are possible to save.
Usher Syndrome
Unlike some of the other rare eye conditions on the list, Usher’s syndrome can also affect the hearing capacities of patients. While quite rare, it is curiously enough the most common condition that affects both hearing and vision. Usher syndrome is related to Retinitis Pigmentosa, but in addition to experiencing the symptoms of RP, people with Usher syndrome often have severe balance issues and hearing loss. Severity of the condition is typically broken down into three tiers, depending on the severity of vision, hearing, and balance impairment.
Uveal Coloboma
Because it is one of the most-rare eye conditions, it is not always properly diagnosed. For this reason, the National Eye Institute estimates that Uveal Coloboma occurs in between 0.5 to 2.2 cases per 10,000 births. Coloboma is used to help describe the absence of normal tissue in or around the eye. Consequently, the coloboma can affect the eyelid, lens, macula (handles daylight, fine and color vision), and the optic nerve. Because Uveal Coloboma patients are missing a component of the eye, it is responsible for a significant portion of blindness in newborns. However, not all patients are blind. Depending on the part of the eye affected, people with UC may suffer from mere light sensitivity or a more limited field of vision.
Uveal Coloboma has no cure, but corrective treatments are available for some patients.
Photophobiais a symptom of abnormal intolerance to visual perception of light.
As a medical symptom, photophobia is not a morbid fear or phobia, but an experience of discomfort or pain to the eyes due to light exposure or by presence of actual physical sensitivity of the eyes, though the term is sometimes additionally applied to abnormal or irrational fear of light such as heliophobia.The term photophobia comes from the Greek φῶς (phōs), meaning "light", and φόβος (phóbos), meaning "fear". Photophobia is a common symptom of visual snow.
photon a wave or particle
Light sensitivity, or photophobia, is an intolerance of light. Some only feel discomfort from bright lights, while others in extreme cases can not stand any type of light. Sources can range from sunlight, fluorescentlight, incandescent light or flames of candles or fires. Some people tend to squint or close their eyes if their sensitivity is too strong. There are many different reasons why someone could have a sensitivity to lights, but the biggest issue is the underlying cause, as photophobia is a symptom, not a condition or disease.Photophobia is known to happen to all ages, young and old.
Photophobia is classified as an extreme sensitivity to light. Photophobia is not a disease on its own. It is usually a symptom caused by another condition. It can be extremely painful, frustrating and debilitating at times.
When exposed to bright light, look for the following:
the inability to be in the sun without squinting
searching out dark or shady areas for relief
nausea or dizziness
headaches or migraines
eye pain
Some of these symptoms can be normal if they are mild and are not associated with pain. If they become significant enough that you avoid the sun or alter your habits, it is time to see a doctor.
Symptoms of Photophobia
There are a few obvious symptoms to recognize your sensitivity to light has increased, such as:
Discomfort
Need to close eyes
Need to squint
Burning
Excessive tearing
In some cases, there might not be any sort of symptoms except the sensitivity to light itself. People have reported nothing one day, then sensitivity the next day. Each individual is unique and experiences different symptoms. Again, it depends on the underlying cause. In other cases, people will suffer many other types of symptoms, depending on the condition or disease that is causing the light sensitivity.
Glare-control sunglasses, like these by Corning, are helpful if you are sensitive to sunlight or even strong indoor lighting.
Causes of Photophobia
There are several different reasons why someone might be suffering from photophobia or sensitivity to light. It’s not a disease, disorder, problem or condition. In fact, it’s a symptom of many different diseases, disorders, problems and conditions. For example, an infection or inflammation that irritates the eyes can cause photophobia. Also, it can be a symptom of an underlying disease such as a viral illness or a severe headache or migraine.
People can be sensitive to light for many different reasons. It doesn’t always occur because of an eye condition, and sometimes there isn’t a cause at all – some people are just more sensitive to light than others.
IPRGC cells or melanopsin cells transduce light into pain.
Some eye diseases cause this symptom, including:
Dry eye
Uveitis (swelling of the inside of your eye)
Keratitis (swelling of your cornea, the clear layer that covers the colored part of your eye)
Iritis (swelling of the colored ring around your pupil)
Cataracts (cloudy coverings over the lenses of your eyes) Corneal abrasion (a scratch on your cornea)
Conjunctivitis (inflammation of the conjunctiva, the clear tissue that sits over the white part of your eye)
Damage to your retina, the light-sensitive layer in the back of your eye Blepharospasm (a condition that makes your eyelids close uncontrollably)
Photophobia may also affect some people who have thesementalhealth conditions:
Agoraphobia(a fear of being in public places)
Anxiety
Bipolar disorder
Depression
Panic disorder
Some things which can make you light sensitive include:
Medicationstaken for other conditions – for example tetracycline (an antibiotic), and digitalis (a drug used for heart problems).
People who suffer or have suffered with migrainestend to be more sensitive to light. Some find that special coloured tinted lenses can help. These coloured lenses are individually prescribed by some optometrists and can also be used to help people who experience glare from pages of text, such as people with dyslexia.
Meningitiscan cause light to become painful quite quickly. If your light sensitivity comes on very suddenly or a child that you’re caring for becomes very light sensitive very quickly, this should be checked straight away by a medical professional in case it is the first sign of this more serious condition. eResearch by Navid Ajamin -- winter 2010
If you begin to experience light sensitivity, have your eyes checked by an optometrist (optician) – they can check that there is no underlying eye condition which may be causing this and may be able to suggest ways to help you cope.
Photophobia preventionat home
Once the underlying cause has been determined, a few practical tips can help minimize photophobia.- Use polarized sunglasses when outdoors
Wear a hat or cap when outdoors
Avoid bright fluorescent lights
Utilize natural light where possible for indoor settings
Control indoor lighting with dimmers and consider replacing any fluorescent or cool white LED light bulbs with a warm white LED light bulb or an incandescent light bulb.
Control the brightness on your screen by adjusting the settings on your TV, computer, phone and other devices
Wear light-filtering lenses or tinted lenses indoors At home is where we have the greatest ability to control our light environment.
Photophobia Treatment
The best treatment for light sensitivity is to address the underlying cause. Once the triggering factor is treated, photophobia disappears in many cases.
If you are taking a medication that causes light sensitivity, talk to your prescribing physician about discontinuing or replacing the drug.
If you're naturally sensitive to light, avoid bright sunlight and other harsh lighting sources. Wear wide-brimmed hats and sunglasses with ultraviolet (UV) protection when outdoors in daylight. Also, consider wearing eyeglasses with photochromic lenses. These lenses darken automatically outdoors and block 100 percent of the sun's UV rays.
For bright sunlight, considerpolarized sunglasses. These sun lenses provide extra protection against glare-causing reflections of light from water, sand, snow, concreteroadways and other reflective surfaces.
In an extreme case, you may consider wearing prosthetic contact lenses that are specially colored to look like your own eyes. Prosthetic contact lenses can reduce the amount of light that enters the eye and make your eyes more comfortable.
Reference:
rnib.org.uk
webmd.com
axonoptics.com
en.wikipedia.org
sciencedirect.com/science/article
allaboutvision.com
michiganheadandneck.com
See also:
GUIDE TO PHOTOPHOBIA / LIGHT SENSITIVITY-- axonoptics.com
Age-related macular degeneration (AMD) results in damaged sharp and central vision. Central vision is needed for seeing objects clearly and for reading and driving. AMD affects the macula, the central part of the retina that allows the eye to see fine details.
Age-related macular degeneration
Vision loss with AMD
Vision loss with cataract
Vision loss with glaucoma
Amblyopia, also referred to as "lazy eye," is the most common cause of vision impairment in children. With amblyopia, the vision in one eye is reduced because the eye and the brain are not working together properly. The eye itself looks normal, but it is not being used normally because the brain is favoring the other eye.
Amblyopia
Strabismus involves an imbalance in the positioning of the two eyes. Strabismus can cause the eyes to cross in (esotropia) or turn out (exotropia).
CDC is the nation's leading science-based, data-driven, service organization that protects the public's health. CDC puts science into action to help children stay healthy so they can grow and learn; to help families, businesses, and communities fight disease and stay strong; and to protect the public's health.
If you see a rapid movement from the corner of your eye, you automatically turn your head. This reflex allows us to react quickly to possible dangers. Test how large your visual field is. Please do not wear spectacles while doing the test.
Visual pathway lesions From top to bottom: 1. Complete loss of vision in the right eye 2. Bitemporal hemianopia 3. Homonymous hemianopia 4. Quadrantanopia 5. & 6. Quadrantanopia with macular sparing
Take a pen or pencil in your right hand and hold it at arm's length in front of your face. Cover your left eye with your other hand. Look straight ahead and maintain your gaze while slowing moving the pen or pencil to the right in an arc movement while keeping your arm outstretched. Stop as soon as the pen or pencil disappears from your visual field. If your visual field is of normal size, your arm should be at an angle of 90° to the position where you started the movement. Now move your outstretched arm to the other side of your body with the same movement until the pen or pencil again disappears from your visual field. The angle should be slightly less, around 60°, because the nose restricts the visual field more on this side. If you have the impression that you are not reaching the angles given, you shouldurgently consult aneye care professional.
A normal visual field is an island of vision measuring 90 degrees temporally to central Fixation, 50 degrees superiorly and nasally, and 60 degrees inferiorly. Visual acuity increases from movement discrimination in the extreme peripheral vision to better than 20/20 in the center of vision.
In order to find and follow glaucoma, visual fields are measured by a computer one eye at a time. One eye is covered and the patient places his or her chin in a type of bowl. Lights of various intensity and size are randomly projected around inside of the bowl.
A visual field test is a method of measuring an individual's entire scope of vision, that is their central and peripheral (side) vision. Visual field testing maps the visual fields of each eye individually and can detect blind spots (scotomas) as well as more subtle areas of dim vision. The visual field test is a subjective examination, so the patient must be able to understand the testing instructions, fully cooperate, and complete the entire visual test in order to provide useful information.
There are a variety of methods to measure the visual fields. During an eye exam, visual field testing is performed one eye at a time, with the opposite eye completely covered to avoid errors. In all testing, the patient must look straight ahead at all times in order accurately map the peripheral visual field. Most modern visual field testing devices also continuously monitor fixation, or the ability of the patient to maintain a consistent straight ahead gaze.Visual field testing is most frequently used to detect signs of glaucoma damage to the optic nerve.
Automated static perimetry test
In addition, visual field tests are useful for detection of central or peripheral retinal diseases of the retina, eyelid conditions such as drooping (ptosis), optic nerve damage and disease, and conditions affecting the visual pathways from the optic nerve to the area of the brain (occipital cortex) where this information is processed into vision.
Who Needs Visual Field Testing?
Visual field testing is an important part of regular eye care for people who are at risk for vision loss from disease and other problems. People with the following conditions should be monitored regularly by their ophthalmologist, who will determine how often visual field testing is needed:
Glaucoma
Multiple sclerosis
Hyperthyroidism
Pituitary gland disorders
Central nervous system problems(such as a tumor that may be pressing on visual parts of the brain)
Stroke
People with diabetes and high blood pressure have a greater risk of developing blocked blood vessels in the optic nerve and retina. They may need visual field testing to monitor any effects of these conditions on their vision.
If your visual field is limited, your ability to drive may be in jeopardy. If you are concerned about vision loss or your ability to continue driving, talk with your ophthalmologist.
What are the different types of visual field tests?
Confrontation visual field testing: The doctor faces the patient and asks the patient look straight ahead. The doctor will present stationary or moving targets in the patient's peripheral (side) visual fields. While maintaining a straight-ahead gaze, the patient lets the doctor know when he/she can see the target in the peripheral vision. The target may be a small disc on a stick, but most commonly the target is the doctor's hand holding up one or two fingers.
Amsler grid: This is a printed image of a grid with a dot in the center. The patient is asked to look at the dot, one eye at a time, and note whether the grid lines surrounding the dot appear distorted, faded, or partially missing. This test is most often used to detect central visual field defects.
Static automated perimetry (such as Octopus or the Humphrey Field Analyzer): Pinpoint flashes of light of varying size and brightness are projected within a large white bowl. The patient is asked to look at the center of the bowl and press a button each time a light is seen in the peripheral vision. The machine collects the data and uses sophisticated software to analyze the results.
Kinetic perimetry (such as Goldmann perimeter): Moving targets of various light sizes and intensities are shown and the patient indicates when they become visible in the peripheral vision. The resulting data is used to map the full visual field. The full, normal range of the visual field extends approximately 120° vertically and a nearly 160° horizontally.
Frequency doubling perimetry: This test utilizes varying intensities of a flickering image to analyze the visual field. It is particularly useful in detecting early glaucoma field loss.
Visual field testing can be performed clinically by keeping the subject's gaze fixed while presenting objects at various places within their visual field. Simple manual equipment can be used such as in the tangent screen test or the Amsler grid. When dedicated machinery is used it is called a perimeter.
The exam may be performed by a technician in one of several ways. The test may be performed by a technician directly, with the assistance of a machine, or completely by an automated machine. Machine based tests aid diagnostics by allowing a detailed printout of the patient's visual field.
Other names for this test may include perimetry, Tangent screen exam, Automated perimetry exam, Goldmann visual field exam, or the Humphrey field exam.
Vision therapy is has been shown over decades to successfully play a role in the management of several conditions, including;
Lazy eye
Eye turns (strabismus)
Convergence Insufficiency
Dyslexia
ADHD
Learning difficulties
Who benefits fromvision therapy?
Many people can benefit from vision therapy. Some of the most common groups of people who may benefit from vision therapy include:
Children with visual problems such as amblyopia (lazy eye), strabismus (crossed eyes), and visual perception disorders like dyslexia.
Adults with visual problems such as binocular vision disorders (double vision, convergence insufficiency), acquired brain injuries, and visual problems caused by trauma.
Athletes of all ages who want to improve their visual skills, such as hand-eye coordination, reaction time, and visual tracking, in order to enhance their sports performance.
People who have suffered from a stroke or have been diagnosed with neurological conditions such as multiple sclerosis, traumatic brain injury, or cerebral palsy.
Individuals who experience visual symptoms such as headaches or eye strain caused by visual problems, or those who have been diagnosed with a specific visual disorder such as myopia, hyperopia, or astigmatism.
People who have had cataracts or other eye surgery and need to rehabilitate their vision.
Individuals who have reading difficulties, difficulty with eye-hand coordination, or those who are experiencing difficulties in school or at work due to visual problems.
It’s worth noting that vision therapy is not a one-size-fits-all solution and not everyone will benefit from it. An eye examination and consultation with a vision therapist are necessary to determine if vision therapy is appropriate and beneficial.
Also Read: What is Vision Therapy? How is it helpful in treating Vision Problems?
What are the principles of vision therapy?
Vision therapy works by targeting specific areas of the visual system, including the eyes, the brain, and the nerves that connect them. The therapy includes a variety of exercises and activities that focus on improving visual skills such as eye coordination, focusing, and tracking.
What is vision therapy?
Vision therapy is a program that aims to improve a person’s visual abilities. It uses a variety of ways – such as eye exercises, testing, occlusion (patching) lenses and prisms – to treat a range of visual problems.
Vision therapy may be used to treat problems such as:
amblyopia (lazy eye)
eye alignment and coordination problems (including turned eyes or squints)
Each program is designed to suit the specific needs of the individual.
How vision works
Vision is the process of deriving meaning from what is seen. It is more than simply the ability to distinguish fine details (visual acuity). Vision also involves:
accommodation (focusing)
convergence (eye aiming)
binocularity (eye coordination)
fixation and eye movement abilities
eye-hand coordination
visual form perception.
Vision continues to develop after birth and is influenced by the visual environment and someone's experience.
Vision problems can exist even if you have healthy eyes and can see clearly. Difficulties may occur in your eye muscle control and coordination.
If you have vision problems, you may experience visual discomfort when performing visually demanding activities.
How does vision therapy treat eye problems?
According to the Australian Bureau of Statistics
, approximately half the Australian population has some vision problem that requires treatment.
While most people have refractive errors (such as short-sightedness, long-sightedness, astigmatism and presbyopia), in some, their eye problems can be improved by vision therapy.
Although vision therapy is available to people of all ages, it is more effective in children and young adults.
Vision therapy for children and young people
One common problem in children is they may have difficulty coordinating their eyes. To see something clearly, both eyes must be aimed correctly and focused at the right distance.
Any problems with aiming or focusing the eyes can cause a variety of symptoms, including:
intermittent double vision
blurred vision
headaches
eyestrain.
Children with these problems often do not complain about them, but may simply avoid tasks (such as reading), which are difficult or cause discomfort.
An optometrist may suggest a program of vision therapy to improve eye coordination and focusing.
What does a vision therapy program involve?
A vision therapy program (also known as visual training) is designed by an optometrist to meet individual needs. So, your program may differ from someone else’s.
Vision therapy is typically used to improve the coordination and control of eye movements and a program may include:
diagnostic tests
training procedures
exercises
use of lenses and prisms – these may be integral to the successful treatment of your vision problem.
The frequency of optometrist visits, amount of home training and duration of the therapy will depend on the nature and severity of your eye problem.
Sometimes you will work with the optometrist in their office and then other times, you may have work to do at home (such as activities and exercises).
Regular practice is important to achieve the best results. Therapy will teach you how to have better eye control to improve your understanding of what you are seeing and reading. You may find that therapy gives you greater confidence and improves your performance in daily activities – such as at school, university, or work.
وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.


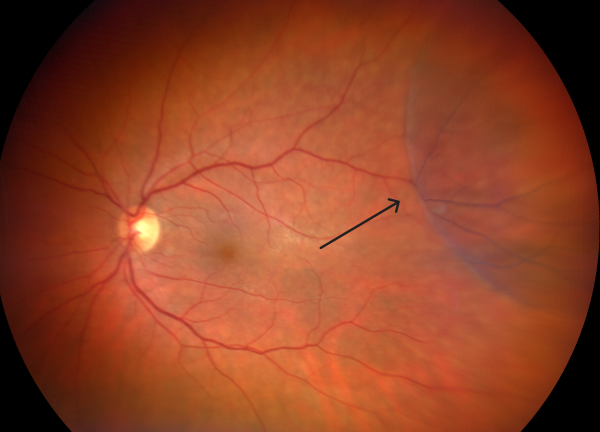


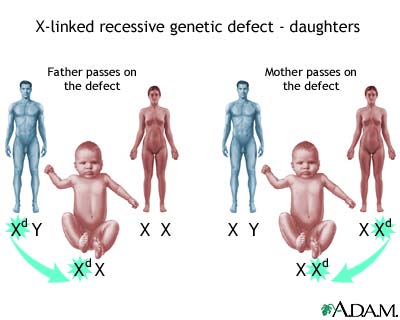

:max_bytes(150000):strip_icc()/Parents-Blurry-Vision-Pregnancy-207bb2797209420d915dc2ccc4f57ba8.jpg)
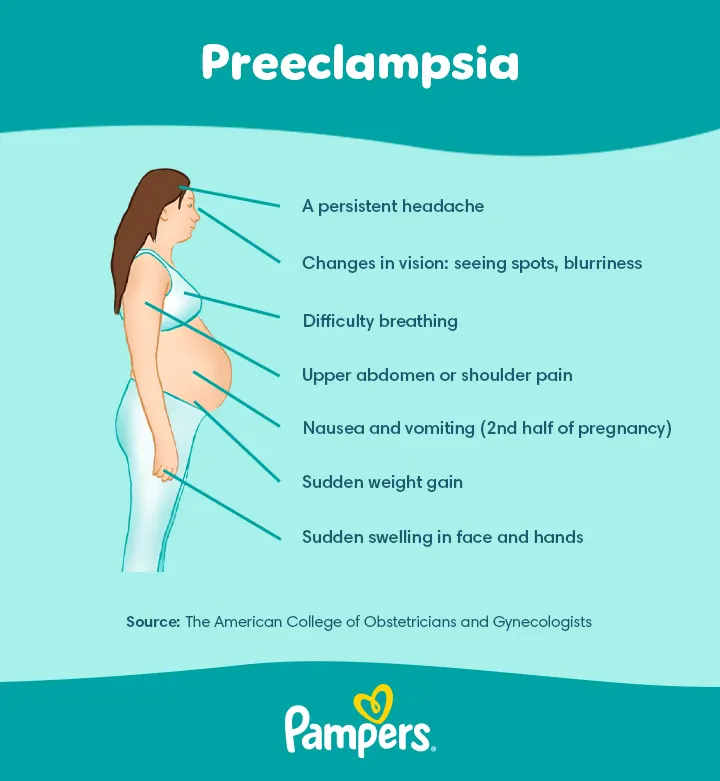



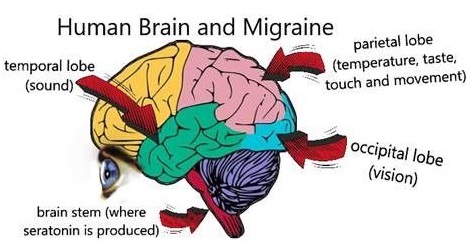

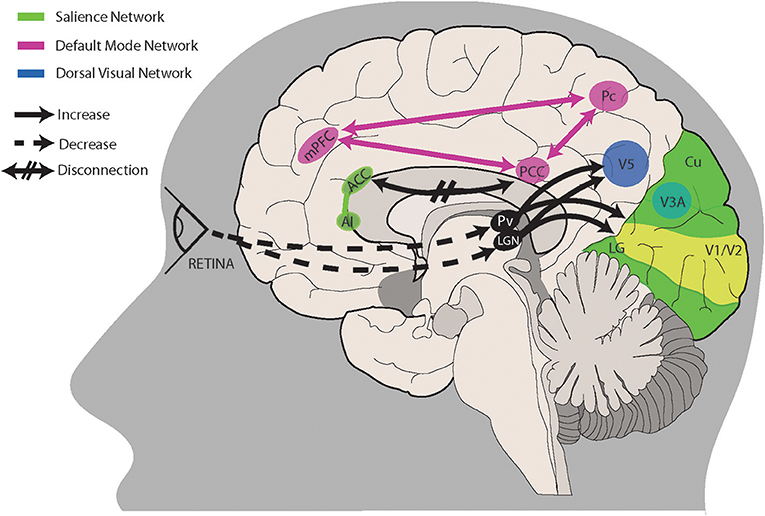

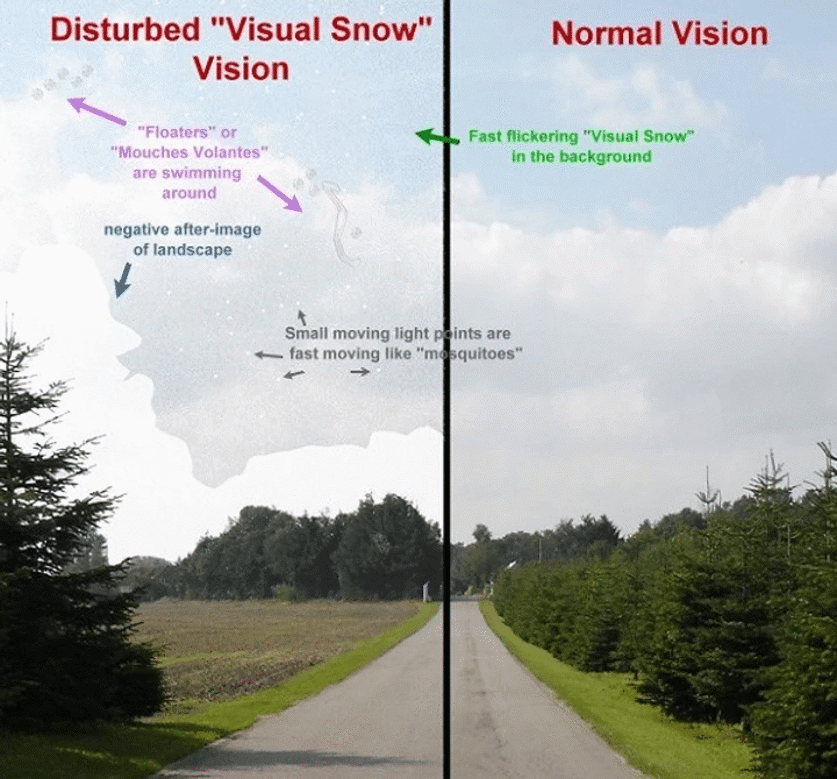


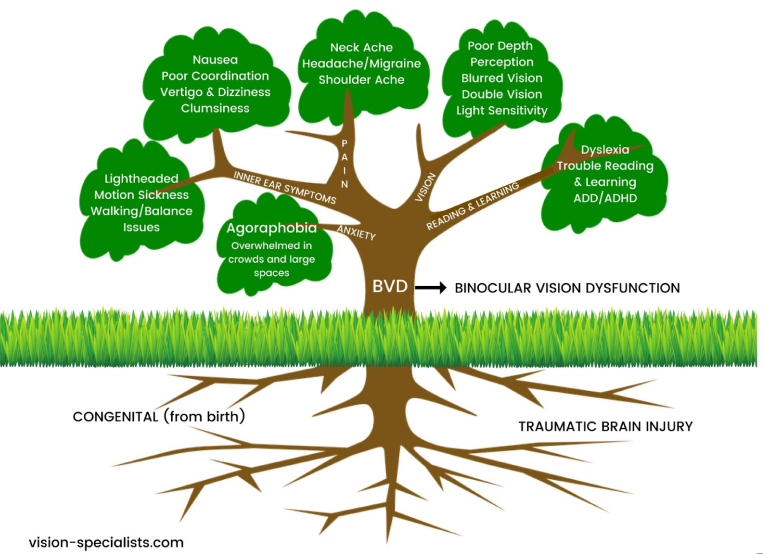


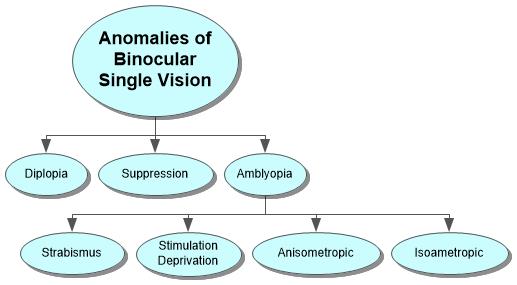



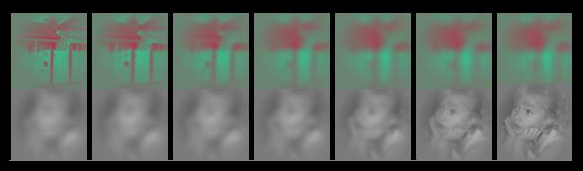

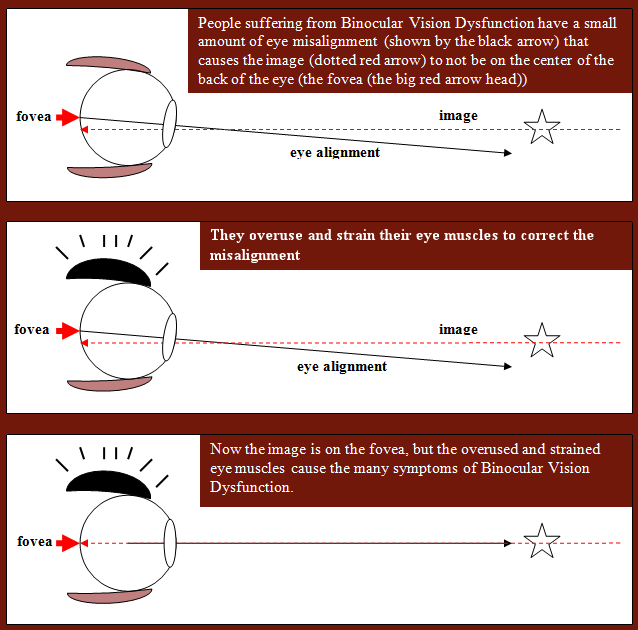



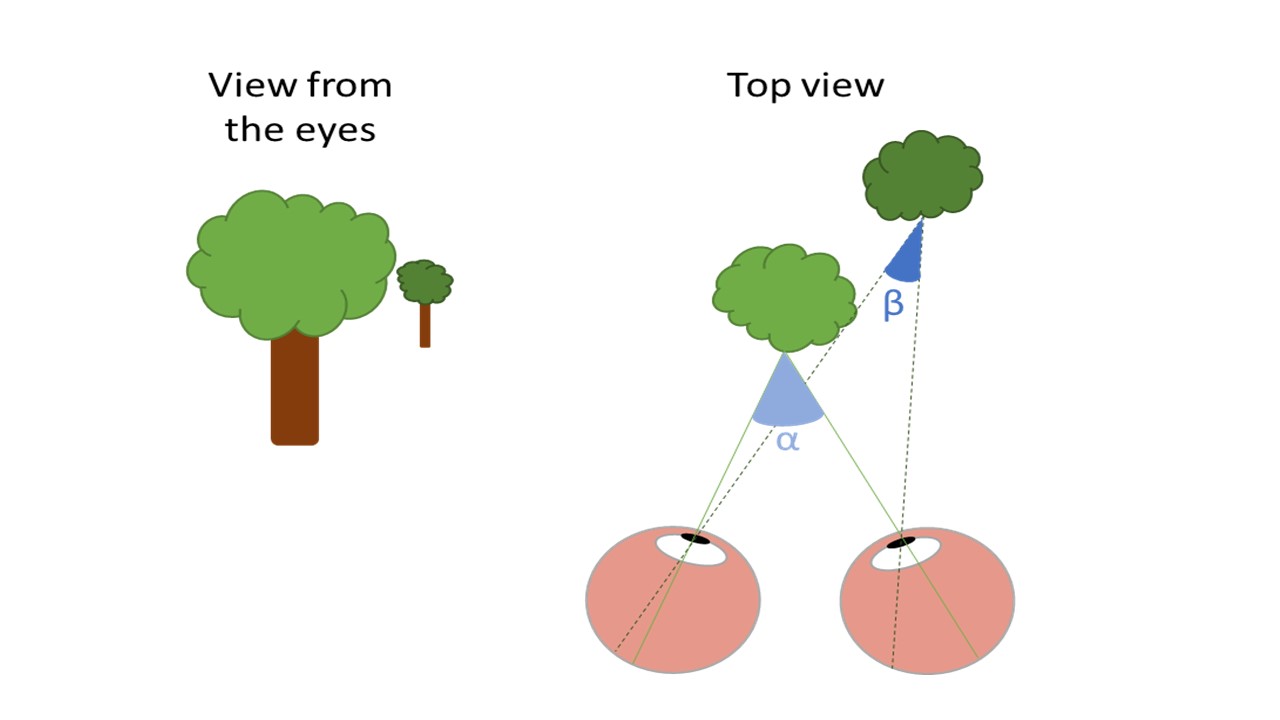



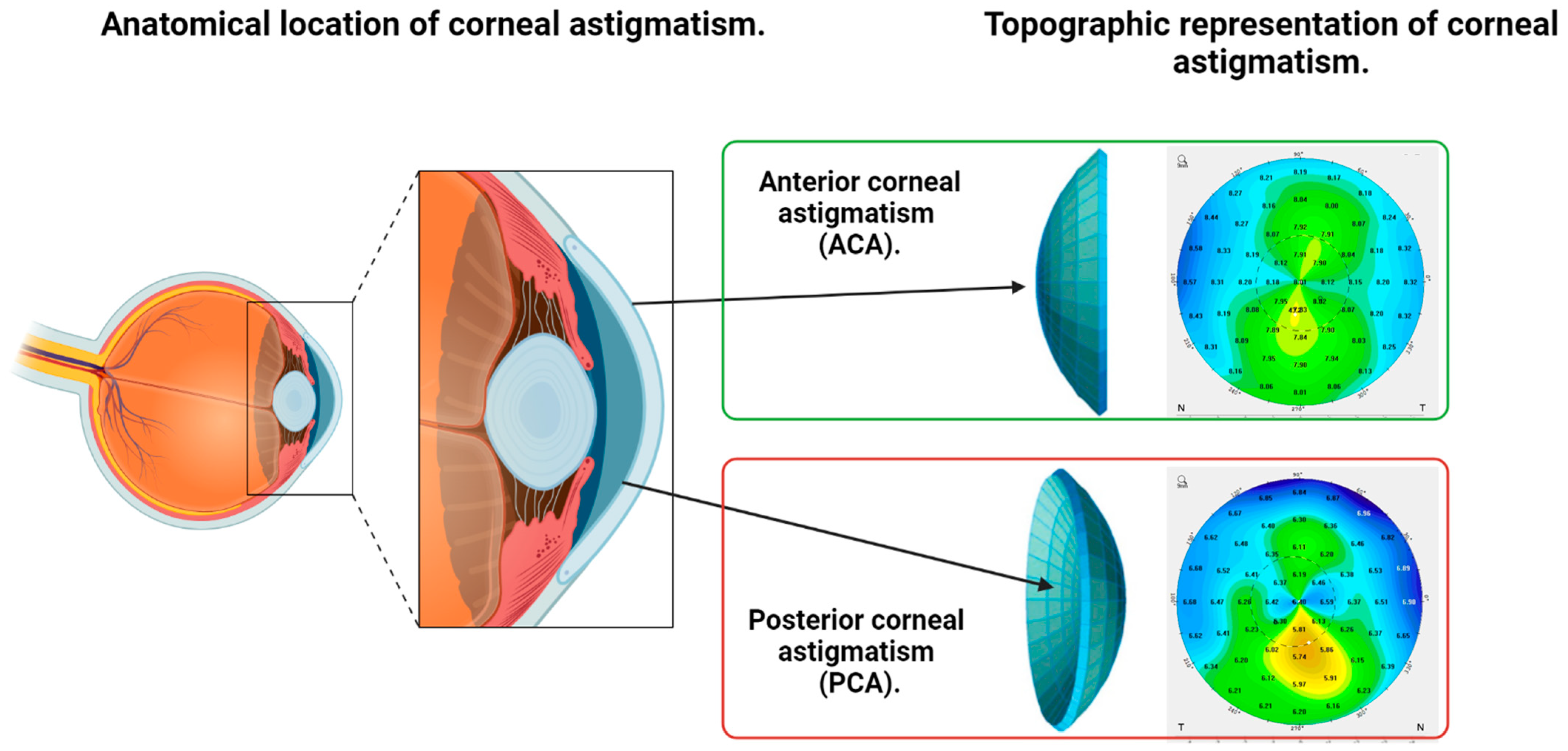

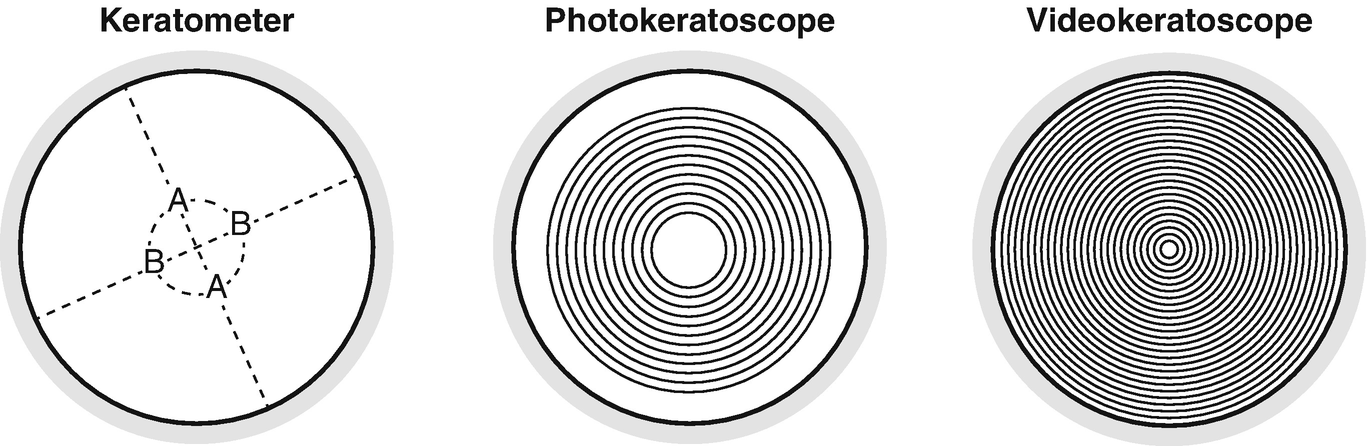


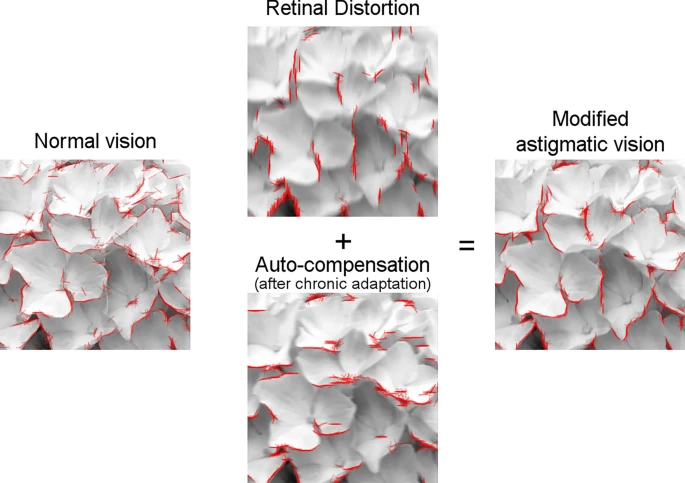











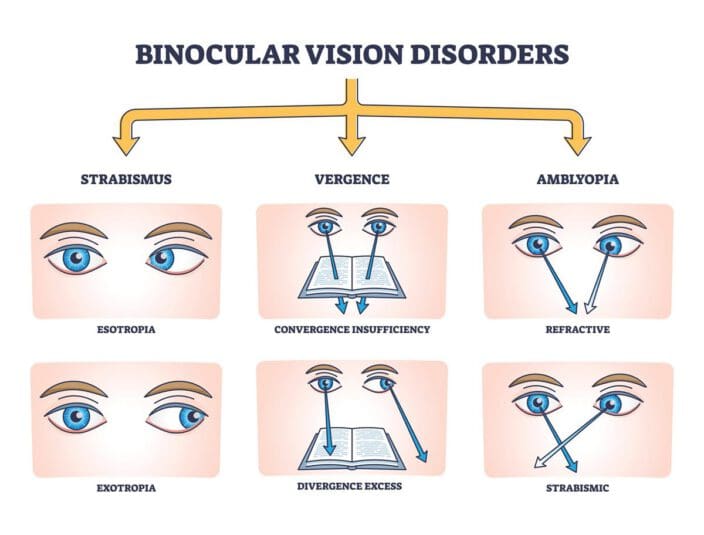




/blurred-vision-56af36f53df78cf772c1a464.jpg)
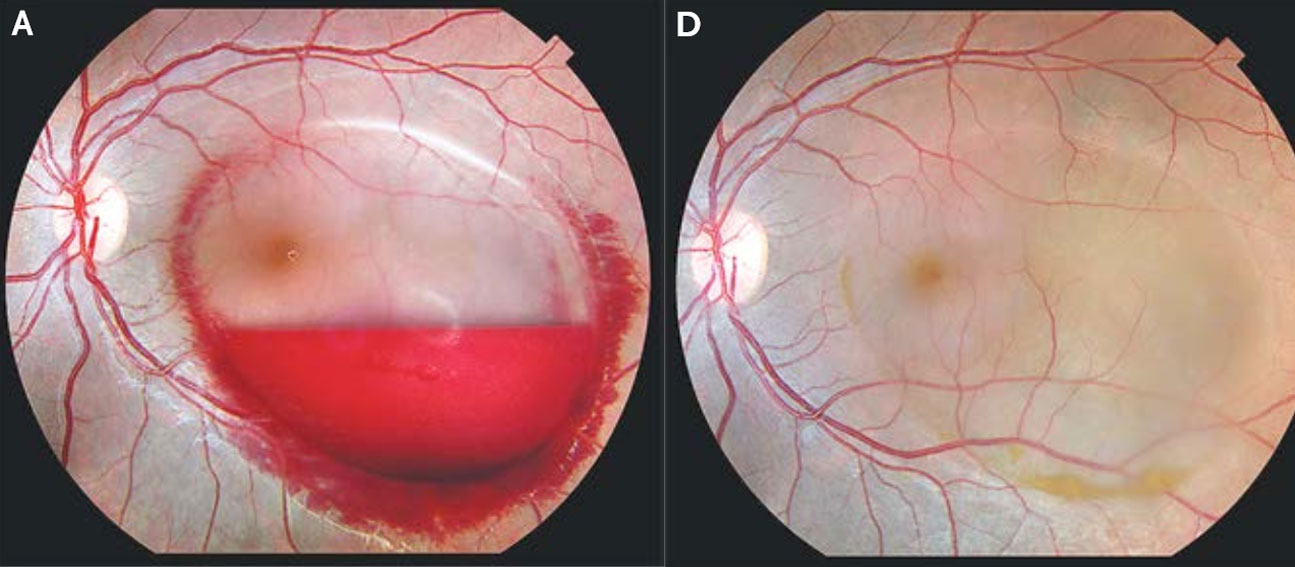



:max_bytes(150000):strip_icc()/Parents-Blurry-Vision-Pregnancy-207bb2797209420d915dc2ccc4f57ba8.jpg)








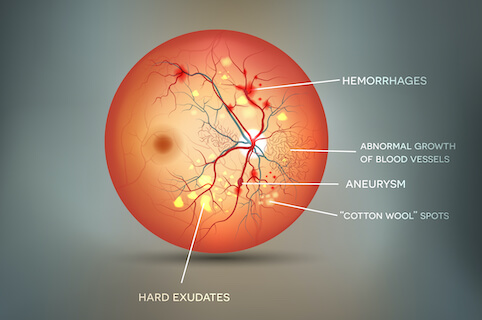

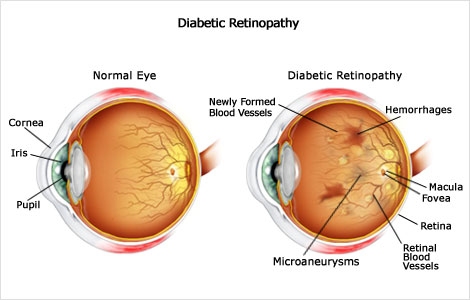




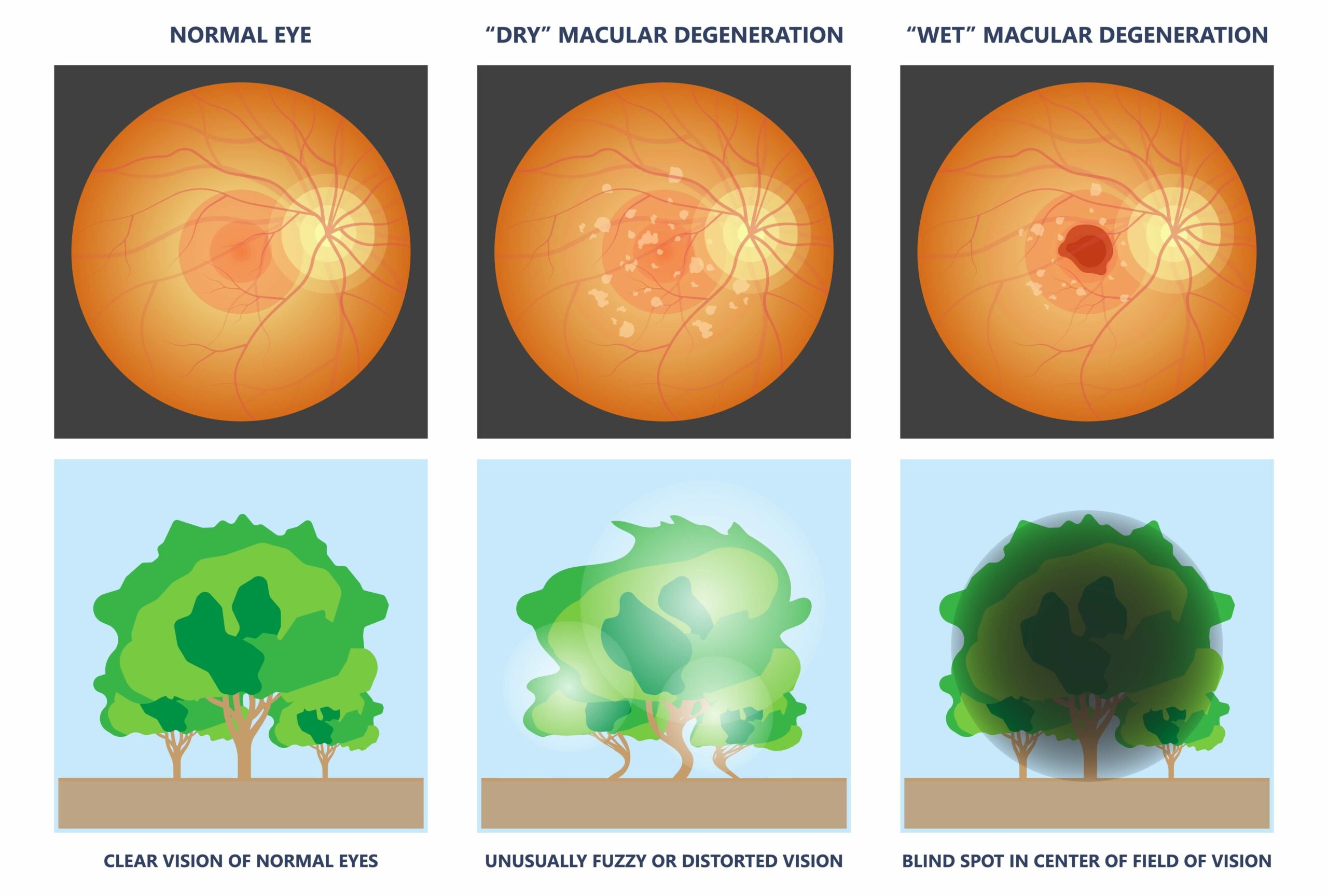

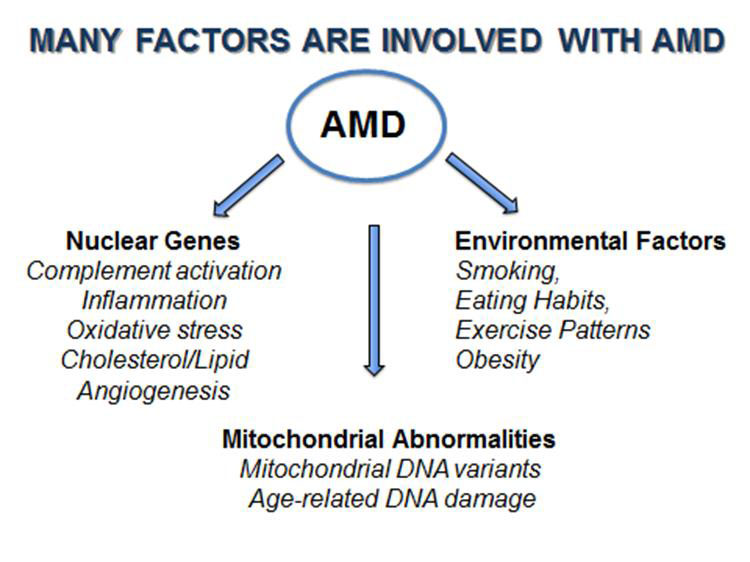

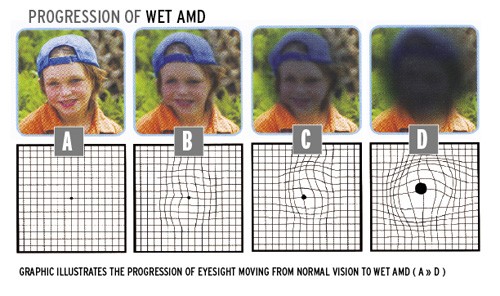
:max_bytes(150000):strip_icc()/VWH_Illustration_Home-Remedies-and-Lifestyle-Changes-for-AMD_Illustrator_Michela-Buttignol_Final-afd2b2bd5d6743e5a473d4846f6573cd.jpg)
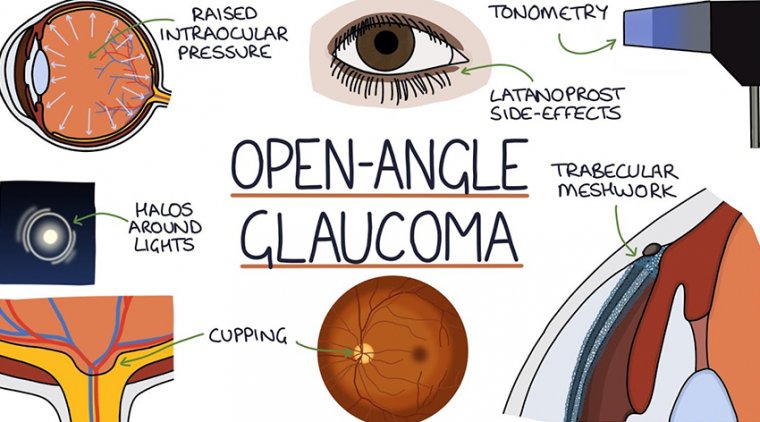






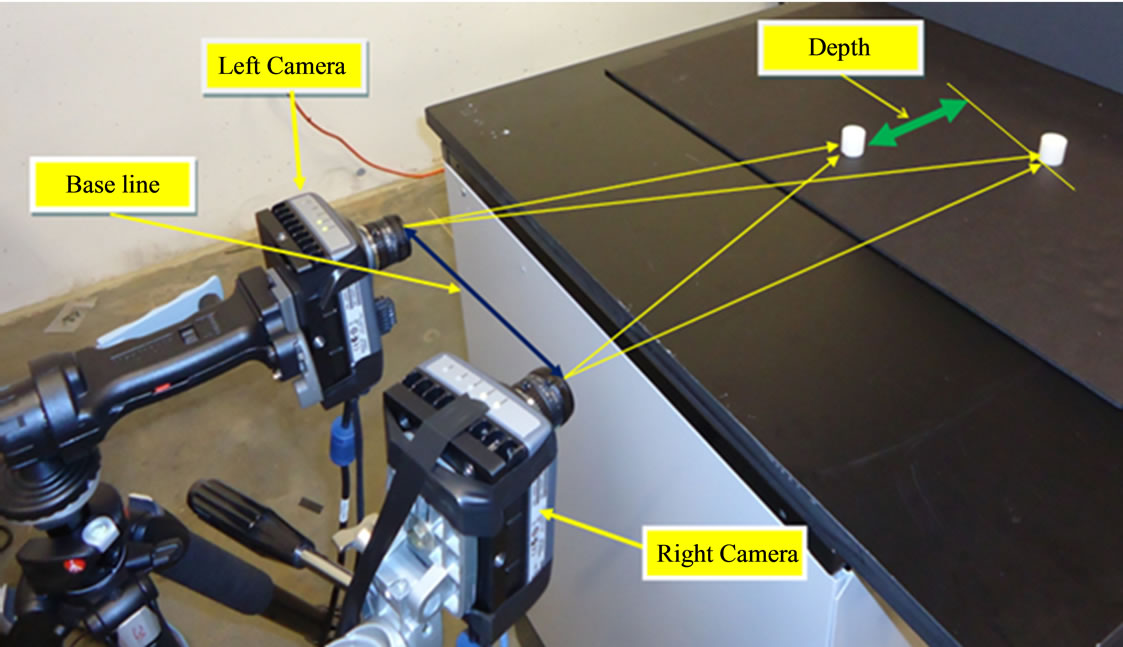


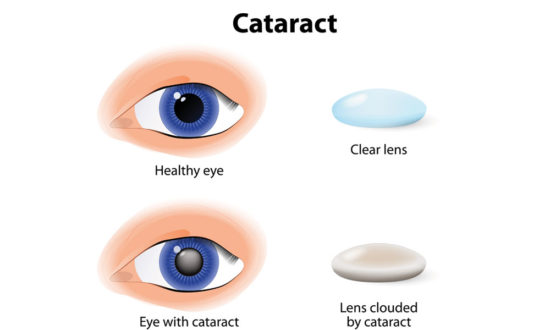

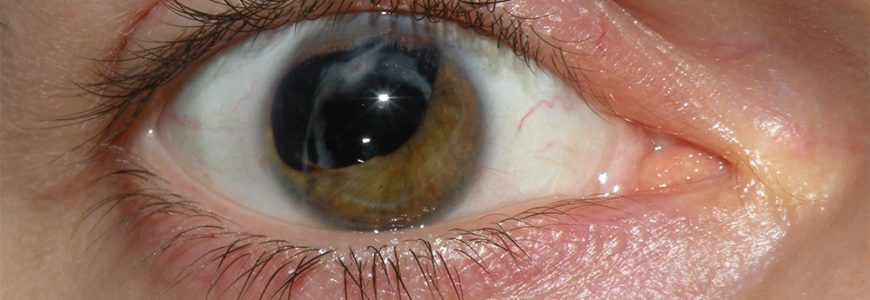


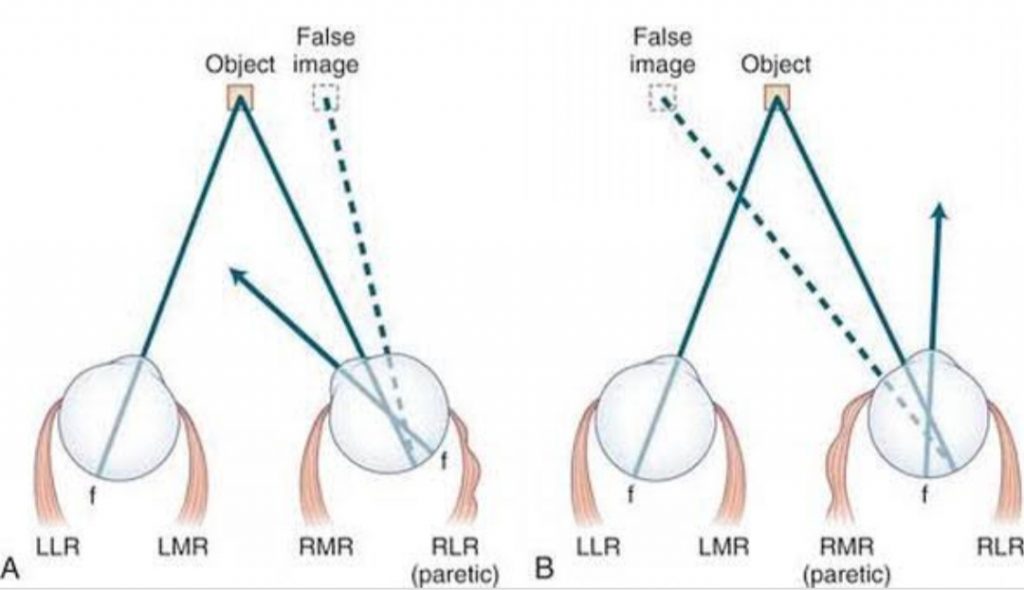




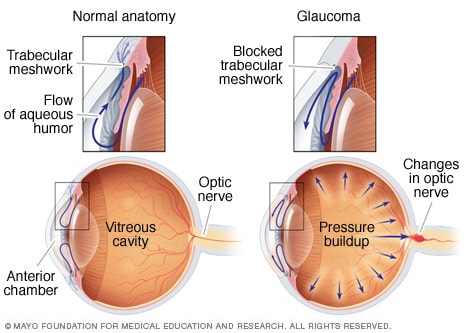






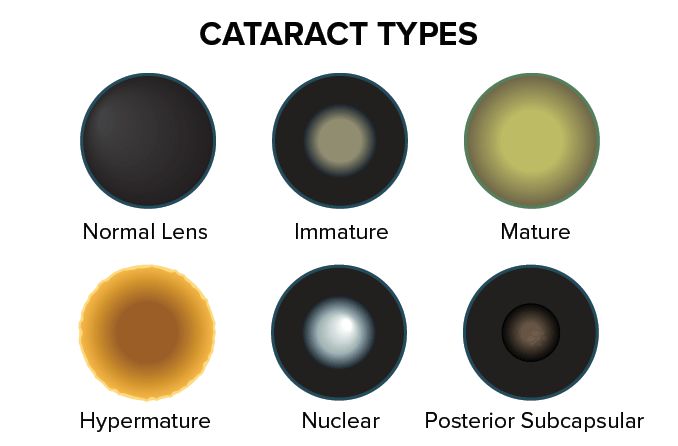






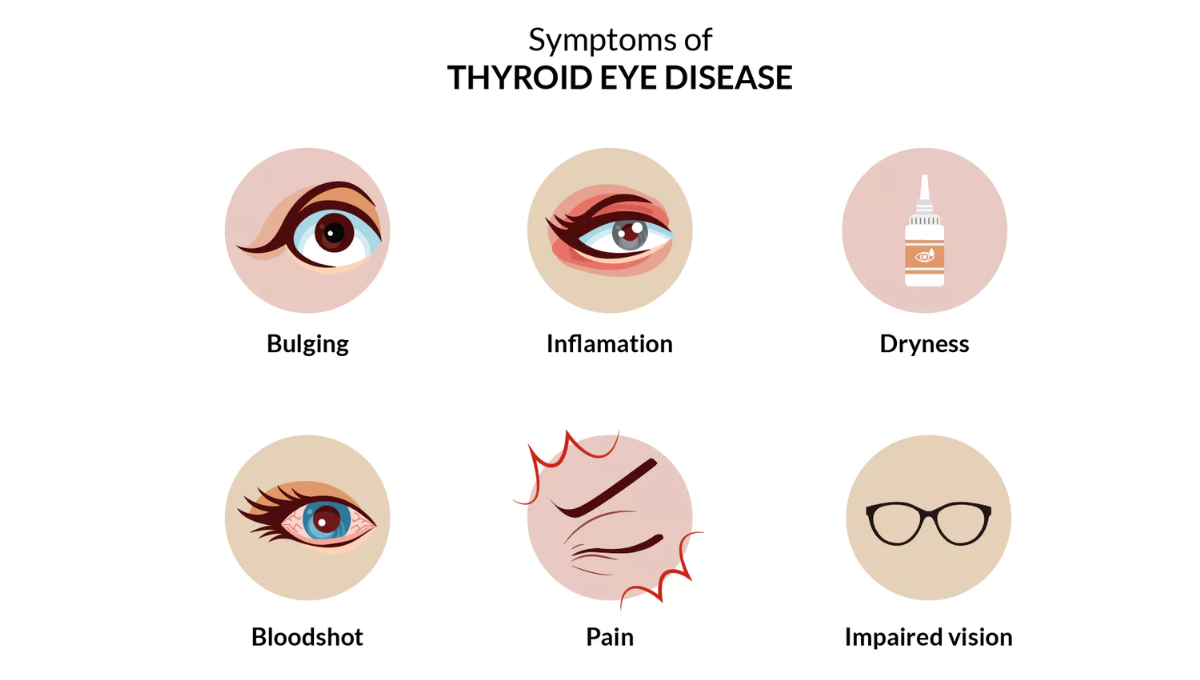




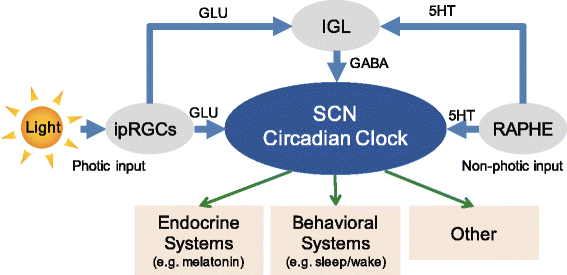







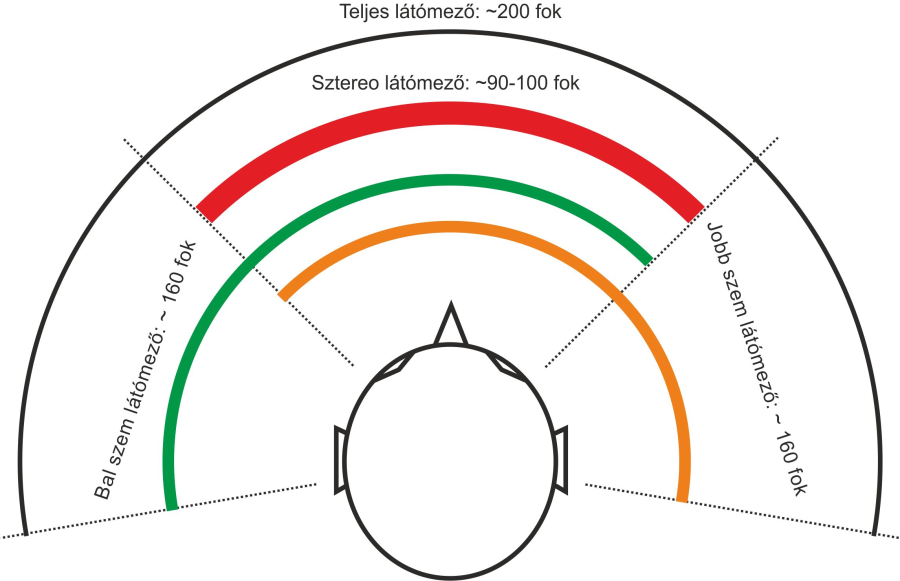



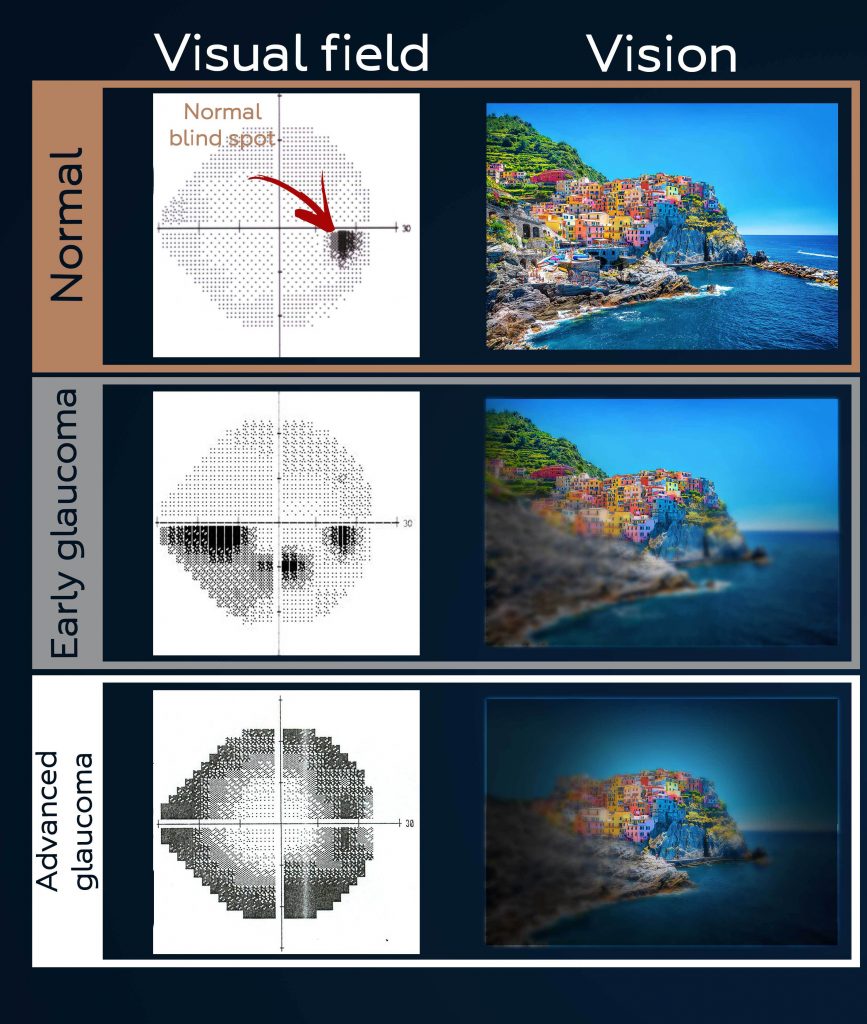





 وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.
وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.