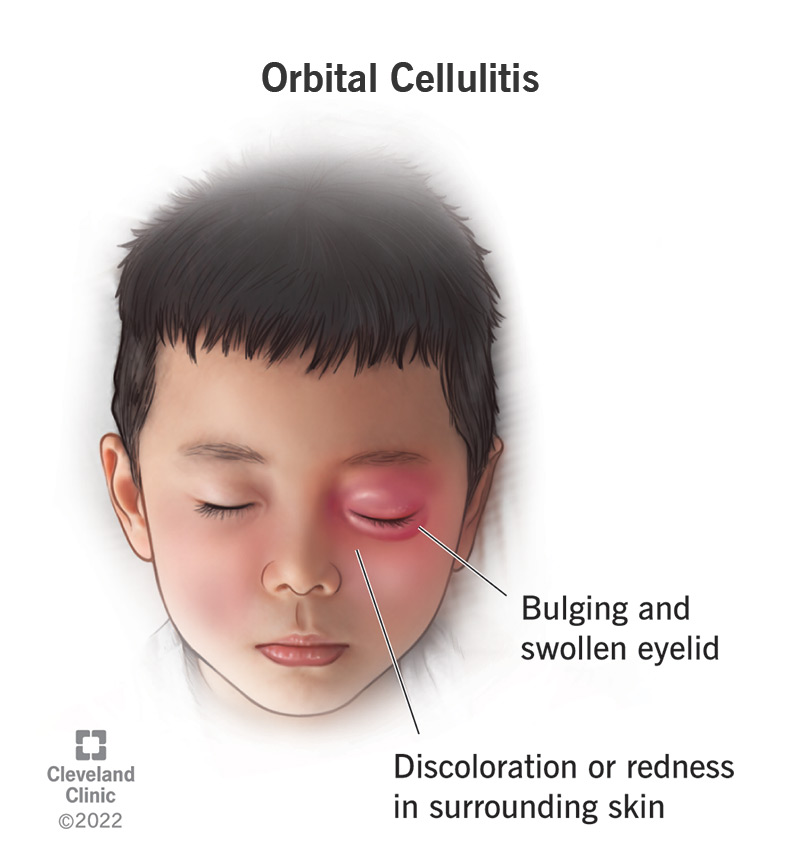
سلولیت اربیتال، عفونت بافتهای نرم و چربی است که چشم را در حفره خود نگه میدارد. سلولیت اربیتال باعث ایجاد علائم ناراحت کننده و دردناک میشود. سلولیت اربیتال مسری نیست و هرکسی ممکن است به این عارضه مبتلا شود اما بیشتر کودکان را تحت تاثیر قرار میدهد. در صورتی که سلولیت اربیتال درمان نشود، میتواند موجب نابینایی شود.
Orbital cellulitis (Periorbital Cellulitis) is an infection that involves the eye and the eye structures within the bony cavity of the face. Both conditions are serious and require immediate medical attention from your child's physician.
Complications can include meningitis, loss of vision, or brain abscess.
What are orbital cellulitis and periorbital cellulitis?
The terms orbital cellulitis and periorbital cellulitis refer to an inflammation and infection of the tissue and skin surrounding the eye. Periorbital cellulitis involves the area from the skin of the eyelid to the bony area that encloses the eye. Orbital cellulitis is an infection that involves the eye and the eye structures within the bony cavity of the face.
Both conditions are serious and require immediate medical attention from your child's physician. Complications can include meningitis, loss of vision, or brain abscess.
Although characterized by swelling around the eye, the eyeball is usually not affected and appears normal.
The most common cause of these types of cellulitis stems from bacterial infection, either by direct trauma or by an infection that spreads from the sinuses.Orbital Infections
Symptoms & Causes
What are the symptoms of periorbital cellulitis?
Although each child may experience symptoms differently, the most common symptoms of periorbital cellulitis appear abruptly and may include:
Swelling of the upper and lower eyelid
Redness of the upper and lower eyelid
Pain
Fever
General discomfort of the eye
The eyeball is usually not affected and appears normal.
Although each child may experience symptoms differently, the most common symptoms of orbital cellulitis appear slowly and may include:
Swelling of the upper and lower eyelid
Swelling and bulging of the eyeball
Decrease in the child's ability to move the eyeball
Decrease in vision
Fever
General discomfort
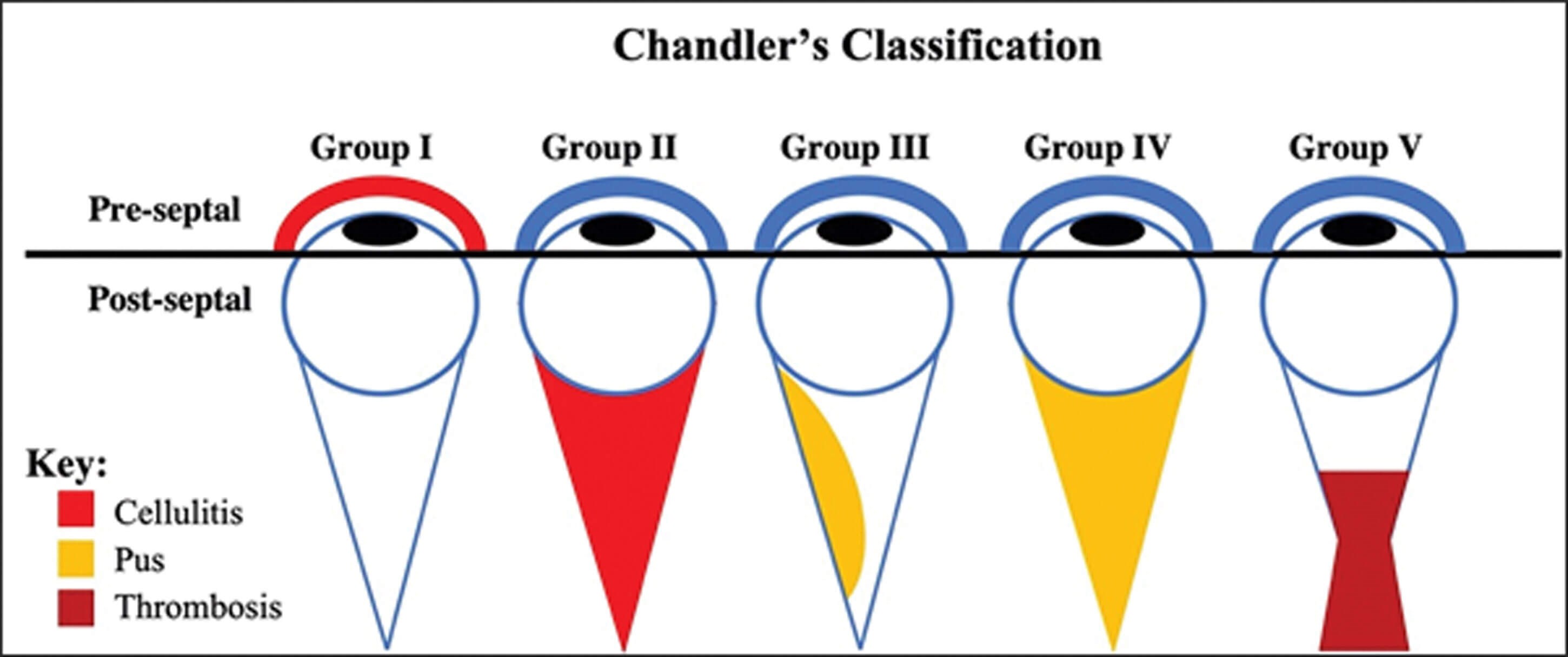
Periorbital (preseptal) and orbital cellulitis are infections of the subcutaneous tissues of the eye. They are differentiated by the location of the infection. Periorbital cellulitis refers to infection of the eyelid and subcutaneous tissues anterior to the orbital septum, whereas orbital cellulitis relates to infection of tissues posterior to the orbital septum. The degree and severity of infection is further graded by the Chandler’s classification (Figure 1).
Figure 1: Chandler’s Classification for degree of infection and severity in orbital cellulitis.
What causes periorbital/orbital cellulitis?
The most common cause of these types of cellulitis stems from bacterial infection. The bacteria that are usually involved are:
Staphylococcus aureus
Streptococcus pyogenes
Haemophilus influenzae
Bacteria gets into the eye and the surrounding cavity many different ways. The two most common ways the infection gets into the eye include:
Trauma: Direct trauma to the eye can lead to infection from the bacteria.
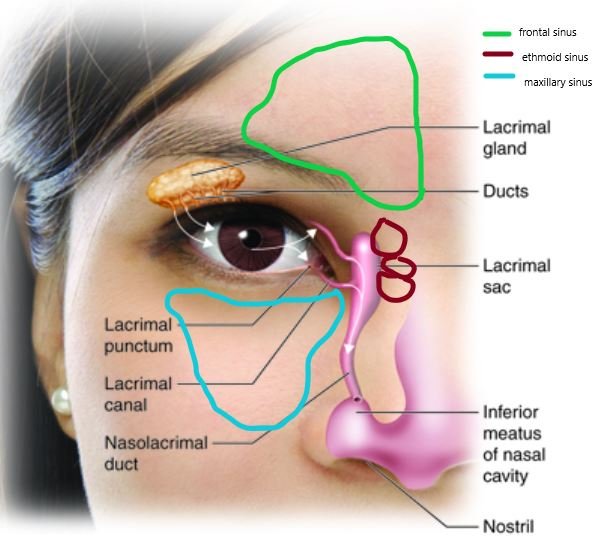
Spread from other areas: Most commonly, the infection begins in the sinuses. The sinuses are cavities, or air-filled pockets, that are near the nasal passage.
تبخال چشمي يک عفونت عود کننده ويروسي است که ناشي از آلودگي با ويروس تبخال ساده است. اين بيماري شايع ترين علت کوري ناشي از بيماري هاي قرنيه اي در آمريکاست در حاليکه در کشورهاي جهان سوم و از جمله ايران شايع ترين علت کوري قرنيه اي، بيماري تراخم است؛ گرچه تبخال چشمي در ايران نيز شايع است. بر اساس مطالعات موجود، اگر فردي يکبار دچار تبخال چشمي شود، به احتمال 50% شانس عود دارد. اين گرفتاري مجدد ممکن است هفته ها يا حتي سالها پس از گرفتاري اوليه بروز کند.
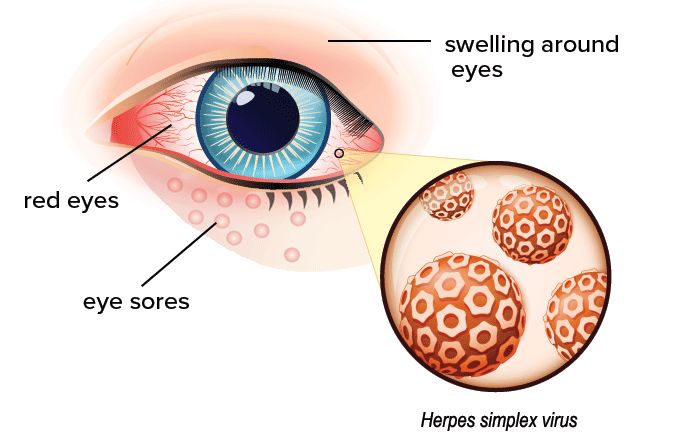
عفونت چشمی ویروس Herpes معمولاً یک چشم را درگیر می کند و یک طرفه است.
تبخال چشمي مي تواند توليد يک زخم دردناک روي پلک و يا سطح چشم کند و باعث التهاب و ورم قرنيه شود. درمان سريع با داروهاي ضد ويروس از تکثير ويروس و تخريب سلولهاي اپيتليال قرنيه ( لايه سلولهاي سطح قرنيه ) جلوگيري مي کند. به هر حال عفونت مي تواند به لايه هاي عمقي تر قرنيه منتشر شده و باعث گرفتاري شديد تر يعني گرفتاري استروماي قرنيه (بستر قرنيه ) يا در اصطلاح کراتيت استرومايي شود که منجر به فعال شدن سيستم ايمني بدن و تهاجم آن به قرنيه و انهدام سلول هاي استروماي قرنيه مي شود. درمان کراتيت استرومايي (عفونت بستر قرنيه ) نسبت به گرفتاري سطحي قرنيه مشکل تر است. حملات عود کراتيت استرومايي مي تواند منجر به اسکار (نسج جوشگاه) قرنيه شود که باعث کدورت قرنيه، کاهش بينائي و حتي کوري مي شود.
Herpes simplex ophthalmia neonatorum
علایم و نشانه های بیماری عفونت تبخال چشمی :
قرمزی در چشم عمدتا در اطراف قرنیه
حساسیت به نور
کاهش بینائی
اشکریزش
درد
Eye Herpes: Symptoms, Treatment & Prevention
تفاوت تبخال چشمی و گل مژه:
تبخال چشمی: Ocular Herpes Simplex
ناشی از عفونت ویروس هرپس سیمپلکس نوع ۱ است.
باعث ایجاد ضایعات پوستی تبخال-مانند در پلکها و اطراف چشم میشود.
همراه با سوزش، خارش، قرمزی و التهاب چشم است.
در موارد شدید، ممکن است به قرنیه چشم نیز آسیب برساند.
گل مژه: stye یا hordeolum
ناشی از عفونت باکتریایی در مجرای غدد پلکی است.
باعث تورم، قرمزی و درد در محل مژهها میشود.
معمولا به شکل تورم کوچک در لبه پلک ظاهر میشود.
در اغلب موارد، فقط پلک درگیر است و عوارضی برای چشم ندارد.
تشخیص بیماری عفونت تبخال چشمی چگونه صورت می گیرد؟
این عفونت به وسیله slit Lamp قابل تشخیص است. ممکن است برای تشخیص دقیق تر، پزشک از قطره های چشمی استفاده کند. در این عفونت معمولاً یک زخم کوچک در قرنیه دیده می شود که به صورت Dendritic یعنی شاخه شاخه است (یعنی زخم به صورت گرد و با حدود مشخص نیست بلکه به [نمای شماتیک زخم دندریتیک قرنیه در افراد مبتلا به کراتیت هرپسی] صورت درختی با شاخه های زیاد می باشد).
درمان بیماری عفونت تبخال چشمی چیست؟
درمان این بیماری بسته به شدت آن دارد. اولین عفونت چشمی ناشی از این ویروس معمولاً با استفاده از قطره ها و پمادهای چشمی و گاهی داروهای ضد ویروسی خوراکی درمان می شود. پزشک ممکن است نواحی آسیب دیده را با ملایمت توسط یک اپلیکاتور که انتهای آن از کتان است، از روی چشم بردارد. در افرادی که به طور مکرر دچار عفونت چشمی Herpes می شوند قرنیه که یک بافت شفاف است تبدیل به یک شیشه مه گرفته می شود و ممکن است برای بهبود دیدشان و برطرف کردن اسکار باقی مانده از این عفونت، نیاز به پیوند قرنیه پیدا کنند. اگر لایه های عمقی قرنیه گرفتار شده باشد، ممکن است که چشم پزشک علاوه بر موارد بالا از قطره های کورتیکواستروییدی(کورتون) نیز استفاده کند که باعث کاهش التهاب می شوند. به خاطر داشته باشید که استفاده از قطره های کورتیکواستروییدی باید با نظارت دقیق پزشک صورت گیرد در غیر این صورت آسیب های جدی به چشم وارد می کند. eResearch by Navid Ajamin -- spring 2013
Herpes Eye Infections
برای جلوگیری از عود مجدد بیماری عفونت تبخال چشمیچه اقداماتی صورت می گیرد؟
اگر عفونت های چشمی ویروس هرپس به صورت عود کنند باشد( یک بار در سال یا بیشتر) معمولاً پزشک توصیه می کند که روزانه دو قرص ضد ویروسی به صورت خوراکی دریافت کنید. بعضی از افراد اظهار می کنند که در معرض نور خورشید قرار گرفتن باعث عود این بیماری می شود که به آنها توصیه می شود حتماً از عینک های آفتابی استفاده کنند.
تبخال چشمي مثل ساير عفونت هاي تبخالي (هرپسي) قابل کنترل است. حدودا 400.000 نفر از مردم آمريکا سابقه گرفتاري با تبخال چشمي را دارند و سالانه 50.000 مورد جديد ديده مي شود که 25% موارد آن از نوع کراتيت استرومايي است. در ايران نيز عفونت هاي تبخالي چشم شايع است ولي متأ سفانه در ايران آمار دقيقي از اين بيماري در دست نيست. در يک مطالعه وسيع، محققان دريافتند که ميزان عود تبخال چشمي طي يک سال 10%، طي دو سال %23 طي 20 سال 63% درصد است. معتقدند که بعضي از فاکتورها نظير: تب، استرس،نور خورشيد و ضربات باعث عود تبخال مي شود.
How do you treat ocular herpes simplex? Treatment for herpes simplex eye infections
You'll usually be prescribed either: an antiviral medicine such as aciclovir, taken as eye ointment, eye drops or sometimes tablets. antiviral medicine with steroid eye drops to reduce swelling.
What is genital herpes?
Genital herpes is an STI caused by two types of viruses – herpes simplex virus type 1 (HSV-1) and herpes simplex virus type 2 (HSV-2).
Oral herpes
HSV-1 often causes oral herpes, which can result in cold sores or fever blisters on or around the mouth. However, most people with oral herpes do not have any symptoms. Most people with oral herpes get it during childhood or young adulthood from non-sexual contact with saliva.
What happens if you have HSV-1?
HSV-1 often causes oral herpes, which can result in cold sores or fever blisters on or around the mouth. However, most people with oral herpes do not have any symptoms. Most people with oral herpes get it during childhood or young adulthood from non-sexual contact with saliva.
Is ocular herpes an STD?
The first thought in most people's mind is venereal disease, sexual transmitted disease (STD). But, in fact most instances of herpes, at least those affecting the eye, are not sexually transmitted, and are not even the type of herpes that is usually associated with sexually transmitted disease.
Does eye herpes ever go away?
Once contracted, the virus stays in the body for life. Ocular herpes tends to infect the cornea, causing inflammation, eye redness, tearing, and — in rare cases — vision loss. Many people with eye herpes may not even know they have it, as it can remain dormant within the nervous system without causing any flare-ups.
Eye herpes is a condition that can happen with very common, highly contagious viruses. Those viruses cause cold sores around your mouth, and chickenpox/shingles elsewhere on your body. These viruses aren’t curable, but treatment can limit their effects, prevent permanent vision loss and avoid future flare-ups.
Herpes simplex eye infections usually affect only one eye.
The symptoms can be similar to some other eye conditions, and can include:
eye pain
a red eye
a swollen eyelid
sensitivity to light
watering of your eye
blurred vision or other changes to your eyesight
blisters or a rash on your eyelid or the skin around your eye
A deeper infection could cause:
Halos around lights
Vision loss
Sensitivity to light
Someone who has never had a herpes infection can only get eye herpes when they come into contact with a fluid or surface infected with a herpes simplex virus.
Most people get first-time infections from someone who has at least one active herpes blister (like a cold sore) on their skin. Less often, you can also get infected by someone whose skin looks normal.
Once someone is already infected, certain things could trigger the virus to wake up again.
These triggers could include:
Stress
Exposure to UV light, either natural (like sunlight) or artificial (like tanning beds)
Heat
A fever
Another illness or injury
A weakened immune system
Menstruation
COVID-19 infection or vaccination
Certain medicines
Sometimes, doctors don't know why the virus reactivates.
تبخال چشمی چگونه درمان میشود؟
درمان این بیماری با روشهای مختلفی مانند تجویز دارو، درمان موضعی، درمان سیستمیک و جراحی ممکن است. تبخال چشمی معمولا با ترکیبی از روشهای زیر درمان میشود که پزشک باتوجهبه شدت بیماری آنها را تجویز میکند:
دارو درمانی:
قطرههای ضد ویروسی مانند آسیکلوویر، والاسیکلوویر یا فامسیکلوویر برای مهار ویروس هرپس
قطره کورتیکواستروئیدی برای کاهش التهاب و درد
قطره آنتی بیوتیک برای پیشگیری از عفونت ثانویه
درمان موضعی:
کمپرس گرم برای تسکین درد و التهاب
استفاده از پماد یا ژل ضد ویروسی روی ناحیه آلوده
درمان سیستمیک:
در موارد شدید یا عود مکرر، داروهای ضد ویروسی خوراکی تجویز میشوند.
داروهای ضد ویروسی خوراکی در موارد نیاز به درمان طولانی مدت
درمان جراحی:
در موارد آسیب شدید قرنیه ممکن است نیاز به پیوند قرنیه چشم باشد.
در موارد ایجاد عوارض مانند زخم قرنیه، جراحی برای ترمیم آن مورد نیاز است.
ورم ملتحمه نوزادیبا علائم قرمزی ، اشک ریزش ، ترشح چشم ، التهاب ملتحمه و پلک زخم و حتی با سوراخ شدن قرنیه مشخص می شود .
چشم صورتی یا التهاب ملتحمه یک التهاب با علل و عوامل ایجادکنندهٔ مختلف در ملتحمهٔ چشمهاست. در این مطلب میتوانید با التهاب ملتحمهٔ چشم در کودکان، علل، عوامل، انواع و درمان آن آشنا شوید.
Neonatal conjunctivitis, also called ophthalmia neonatorum, typically presents during the first four weeks of life. The infection is usually acquired during delivery and is the most common ocular disease in neonates. Typical symptoms are persistent tearing and a mucoid discharge in the inner corner of the eye.
Is newborn eye discharge normal?
It is normal for a baby to have sticky yellow or white discharge in the corner of one or both eyes and can cause the eyelashes to stick together. This can last for several months.
What is the difference between dacryocystitis and conjunctivitis?
Conjunctivitis is characterized by redness, itching, and discharge from the eye. While it shares the symptom of discharge with dacryocystitis, conjunctivitis typically involves more diffuse redness across the conjunctiva and lacks the localized swelling over the lacrimal sac evident in dacryocystitis.
P39.1
ICD-10 code P39. 1 for Neonatal conjunctivitis and dacryocystitis is a medical classification as listed by WHO under the range - Certain conditions originating in the perinatal period .
Is bacterial pink eye spreadable?
Pink eye caused by viruses and bacteria can easily spread from person to person in different ways. You can get pink eye from: Close personal contact, such as touching or shaking hands. Contact with droplets from the air after an infected coughs or sneezes.
Pneumococcal conjunctivitis is a bacterial eye infection that causes symptoms such as redness, discharge, and crusting of the eyelids. It is caused by a type of bacterium called Streptococcus pneumoniae. Streptococcus pneumoniae can cause many other types of infections, including middle ear infections and sinusitis.[9]
Chlamydia trachomatis is an obligate intracellular parasite and has been identified as the most common infectious cause of neonatal conjunctivitis. The reservoir of the organism is the maternal cervix or urethra.
? Is pink eye contagious
التهاب ملتحمه در کودک
التهاب ملتحمه که کنژنکتیویت و چشم صورتی نیز نامیده میشود، یک التهاب بسیار شایع و قابل درمان ملتحمهٔ چشم یعنی غشای شفافی هست که درون پلکها و سفیدی چشمها را پوشانده است. عروق خونی هنگامی که ملتهب میشوند، مشهودتر میشوند و ویژگی مشخصهٔ این عارضه را که صورتی یا قرمز شدن چشم است ایجاد میکنند. التهاب میتواند توسط عفونت، یک مادهٔ آلرژیزا یا دیگر عوامل محرک ایجاد شود. همچنین التهاب ملتحمهٔ ناشی از عفونتهای باکتریایی و ویروسی بسیار مسری هستند.
علائم التهاب ملتحمه در کودک
اگر سفیدی یک یا هر دو چشم کودکتان و لبهٔ پایین هر کدام از پلکهایش قرمز باشد، احتمال دارد که التهاب ملتحمه داشته باشد. در حینی که سیستم ایمنی بدن کودک برای مبارزه با عفونت تلاش میکند، ممکن است چشمانش اشکریزی داشته باشند، چسبنده شوند یا شوره بزنند. به محض اینکه متوجه علائم التهاب ملتحمه شدید، با پزشک کودک تماس بگیرید.
به خاطر داشته باشید مهم است که فوراً درمان آن را شروع کنید، تا از گسترش ویروسها جلوگیری کنید و از عارضهٔ ثانویهٔ نادر عفونت پلک و بافت نرم دور چشم پیشگیری شود. قرمزی خفیف چشمها و کمی ورم پلک در یک نوزاد ممکن است نوع کوتاهمدتی از التهاب ملتحمه باشد که در واکنش به قطرههای چشمی ایجاد میشود که در هنگام تولد به نوزادان میدهند.
دلایل و عوامل التهاب ملتحمه در کودک
Patient education: Conjunctivitis (pink eye)
التهاب ملتحمهٔ چشم دلایل مختلفی دارد که برخی از چند دلیل محتملتر آن میتواند شامل موارد زیر باشد: ویروس: اگر کودک شما مبتلا به التهاب ملتحمه و همچنین علائم سرماخوردگی است، عفونت به احتمال زیاد ویروسی است. ویروسها شایعترین عامل ایجاد التهاب ملتحمه هستند. باکتری: اگر چشمهای کودکتان ترشحات زرد غلیظی ایجاد میکنند که باعث ورم پلکها یا چسبیدن آنها به یکدیگر میشود، احتمالاً علت آن باکتریهایی مانند استافیلوکوکها، استرپتوکوکها یا هموفیلوسها است. همچنین نوعی جدی از التهاب ملتحمه باکتریایی به نام افتالمیا نئوناتوروم وجود دارد که در نوزادانی که در طول زایمان مادرشان در معرض کلامیدیا یا سوزاک قرار گرفتهاند بروز میکند. آلرژن: واکنشهای آلرژیک در کودکان زیر یک سال نادر است، اما اگر چشمهای کودکتان خارشدار و متورم و دچار آبریزش و خونگرفتگی هستند و یا آبریزش بینی نیز دارد، ممکن است واکنشی آلرژیک به یک عامل محرک مانند گرد و غبار، گرده یا دود باشد. قطرههای چشمی نوزاد: قطرهٔ چشمی که در هنگام تولد برای جلوگیری از عفونت باکتریایی به نوزاد داده میشود میتواند چشمهایش را تحریک کنند. این عارضه گاهی اوقات کنژنکتیویت شیمیایی نامیده میشود. مجاری اشکی مسدود: حداقل ۲۰ درصد از نوزادان در حالی متولد میشوند که یک یا هر دو مجرای اشکی آنها به طور کامل یا جزئی مسدود شدهاند. این انسداد میتواند منجر به علائمی شبیه التهاب ملتحمه مانند ترشحات سفید یا زرد یا یک التهاب ملتحمه تمامعیار شود. عوامل دیگر: هر چیزی که بتواند چشم و پوشش داخلی پلکها را تحریک کند، از مه یا دود، گرفته تا کلر موجود در استخر شنا میتواند باعث ایجاد این التهاب شود. eResearch by Navid Ajamin -- spring 2012
درمان التهاب ملتحمه در کودک
اگر نوزادتان التهاب ملتحمه دارد، بلافاصله با پزشک خود تماس بگیرید. التهاب ملتحمه میتواند برای یک نوزاد عفونتی جدی باشد. پزشک چشمهای کودک را معاینه خواهد کرد و در مورد علائمش سؤال میکند. هرچند درمان با نوع التهاب ارتباط دارد ولی بسیاری از پزشکان توصیه میکنند که برای کمک به پاک کردن هر نوع ترشحاتی در همهٔ انواع التهاب ملتحمه و درمان هر گونه عفونت اولیه یا حتی جلوگیری از عفونت، چند قطره از شیر دوشیدهشدهٔ مادر را چندین بار در روز در چشمهای آسیبدیده بریزید. درمان هر یک از انواع التهاب ملتحمه به شکل زیر است:
التهاب ملتحمهٔ ویروسی: التهاب ملتحمهٔ ویروسی توسط انواعی از ویروسها ایجاد میشود. این نوع کنژنکتیویت معمولاً طی یک هفته یا همین حدود بهبود مییابد. برای درمان نیز پزشک به شما توصیه خواهد کرد که ناحیهٔ درگیر را با شستن چشمهای کودک با آب گرم و پاک کردن ترشحات خشکشده تمیز کنید و لازم است این کار را با ملایمت انجام دهید. اگر چشمهای کودک پس از دو هفته بهبود نیافت، دوباره پزشک را در جریان بگذارید.
گذاشتن کمپرس گرم روی چشم هم ممکن است تسکیندهنده باشد. برای این کار کافی است یک پارچهٔ تمیز را در آب گرم خیس کنید و آن را روی چشمهای کودک خود قرار دهید، برای مثال وقتی در حال شیر خورن است.
التهاب ملتحمهٔ باکتریایی: اگر باکتری عامل بروز التهاب ملتحمه باشد، پزشک پماد یا قطرهٔ آنتیبیوتیکی را تجویز میکند تا برای حدود هفت روز به چشمهای کودکتان اعمال کنید. زدن پماد ممکن است برایتان راحتتر از قطرههای چشمی باشد. برای زدن پماد ابتدا دستهایتان را بشویید و سپس به آرامی پلک پایین کودک را اندکی پایین بکشید و یک خط از پماد را در امتداد آن بمالید. وقتی تیوب را فشار میدهید و کودک چشمهایش را باز و بسته کند، پماد وارد چشمهایش میشود.
اگر هم از قطرهٔ آنتیبیوتیک استفاده میکنید، آن را در گوشهٔ چشم کودکتان بریزید. انجام این کار در زمانی که چشم او بسته است سادهتر خواهد بود. هنگامی که کودک چشمش را باز میکند، دارو وارد چشمش میشود. دستهای خود را قبل و بعد از ریختن دارو در چشمهای کودکتان بشویید. هرگز از داروهای او برای شخص دیگری استفاده نکنید و از قطرهها یا پمادهای قدیمی استفاده نکنید. داروهای قدیمی به احتمال زیاد استریل نیستند و میتوانند عفونت را بدتر کنند.
اطمینان حاصل کنید که کودکتان دورهٔ کامل آنتیبیوتیکهای تجویزشده را حتی بعد از اینکه علائمش از بین رفتهاند، مصرف میکند. در غیر این صورت ممکن است عفونت برگردد. پزشک احتمالاً توصیه میکند چشمهای کودک خود را با آب گرم شستوشو دهید و ترشحات خشکشده را با ملایمت بردارید، زیرا تجمع مایعات عفونی میتواند از اثرگذاری آنتیبیوتیکها بکاهد. گذاشتن کمپرس گرم روی چشم ممکن است تسکیندهنده باشد. یک پارچهٔ تمیز را در آب گرم خیس کنید و آن را روی چشمهای کودک خود قرار دهید، برای مثال در حینی که شیر میخورد.
التهاب ملتحمهٔ آلرژیک: راهحل مقابله با این نوع التهاب این است که مادهٔ آلرژیزا را شناسایی کنید و کودک خود را دور از آن نگه دارید. میتوانید در مورد روشهای مقابله با آلرژی کودک خود را بخوانید. اگر چشمهای کودک او را اذیت میکند، یک کمپرس سرد ممکن است به تسکین التهاب ملتحمهٔ آلرژیک کمک کند.
التهاب ملتحمهٔ شیمیایی: این واکنش به قطرههای چشمی نوزاد است که برای جلوگیری از عفونت به او داده میشود و احتمالاً در حدود ۲۴ تا ۳۶ ساعت طول میکشد.
همچنین به خاطر داشته باشید که التهاب ملتحمهٔ باکتریایی و ویروسی هر دو فوقالعاده مسری هستند. بنابراین، برای جلوگیری از گسترش عفونت، هر بار که مراقبتهای چشم کودک را انجام میدهید، دستهای خود را بشویید. حولهها، لباسها و ملافههای کودک خود را از دیگران جدا کنید و آنها را مرتب بشویید.
شروع ورم ملتحمه می تواند از چند ساعت تا چند هفته بعد از تولد شروع شود .
Pink Eye in Kids: What Every Parent Needs to Know
عوامل ایجاد کننده ورم ملتحمه عوامل باکتریایی یا ویروسی مانند : گونوگوکی ، استاف اورئوس ، کلامیدیا ، هموفیلوس آنفلوآنزا ، پسودوموناس ، استرپتوکوک ، پنوموکوک ، هرپس سیمپلکس می باشند.
در میان این علل سه عامل مهم تر وخطرناک تر است : ورم ملتحمه گونوکوکی ، ورم ملتحمه کلامیدیائی ، ورم ملتحمه با ویروس هرپس سیمپلکس تیپ 2
ورم ملتحمه گونوگوکی :
1-4 روز بعد از تولد شروع می شود و با ترشحات چرکی فراوان ، ورم ملتحمه و تورم پلک ها خود را نشان می دهد از عوارض وخیم وفاجعه آمیز آن زخم وسوراخ شدن قرنیه و و عفونت داخل چشم ( آندوفتالمیت) است . که می تواند به سرعت باعث کوری شود
انواع ورم ملتحمه میکروبی با درمان آنتی بیوتیک قابل درمان است.
ورم ملتحمه کلامیدیائی :
که معمولا 1-2 هفته بعد از تولد شروع می شود با ترشحات چرکی والتهاب ملتحمه و با شدت کمتراز نوع گونوکوکی تظاهر می کند همانند گونوکوک در اثر آلوده شدن چشم نوزاد در هنگام عبور از کانال زایمانی ایجاد می شود و یکی از علل شایع ورم ملتحمه نوزادی است .
جهت پیشگیری از ورم ملتحمه نوزادی در گذشته از نیترات نقره استفاده می شد ولی امروزه برای پیشگیری پماد تتراسیکلین و اریترومایسین به کار می رود .
درمان :
Causes and Treatment for Pink Eye
در نوع گونوکوک ایزوله کردن نوزاد ، درمان وریدی آنتی بیوتیک ، کشت خون وکشت مایع نخاع وکشت از مادر و دادن سفتریاکسون یا سفوتاکسیم و چکاندن قطره های استریل ایزوتونیک نمکی و معاینه دقیق توسط چشم پزشک توصیه می شود.
درنوع پسودومونا ایزوله کردن نوزاد و انجام کشت و درمان داخل رگی سفتازیدیم و جنتامایسین و معاینه دقیق توسط چشم پزشک توصیه می شود.
در نوع استافیلوکوک ایزوله کردن نوزاد وانجام کشت های مختلف و درمان سیستمیک متی سیلین
در نوع کلامیدیا درمان موضعی موثر نیست درمان خوراکی اریترومایسین در 4 دوز به مدت 14 روز چون 20 % عود می کند یک دوره دوم آنتی بیوتیک ممکن است لازم شود .
در سایر باکتری ها چکاندن قطره های موضعی وآنتی بیوتیک های موضعی مثل باسیتراسین ، نئو مایسین ، پلی میکسین ، هر 6 ساعت به مدت 7-10 روز
Conjunctivitis is the term used to describe inflammation of the conjunctiva—the thin, filmy membrane that covers the inside of your eyelids and the white part of your eye (sclera).
Conjunctivitis is most commonly referred to as red or “pink” eye.
The conjunctiva, which contains tiny blood vessels, produces mucus to coat and lubricate the surface of your eye.When the conjunctiva becomes irritated or inflamed, the blood vessels become larger and more prominent, making your eye appear red. Conjunctivitis may occur in one or both eyes.
Bacterial (bak·tee·ree·uhl) conjunctivitis
Symptoms of conjunctivitis include:
inflammation of the eye
increased tearing
soreness of the eye
foreign body sensation
itchiness of the eye
hazy or blurred vision due to mucous or pus
excess mucous (pus)
crusting of eyelashes in the morning.[1]
What causes conjunctivitis?
- Infection is the most common cause. - Allergy is another common cause. For example, many people with hay fever (allergic to pollen) have red and inflamed conjunctiva. - Irritant conjunctivitis sometimes occurs. For example, your conjunctiva may become inflamed after getting some shampoo in your eyes. The chlorine in swimming baths is a common cause of mild irritant conjunctivitis. The rest of this leaflet is about conjunctivitis caused by infection.[2]
What are the most common causes of conjunctivitis in childhood?
Conjunctivitis is an inflammation of the conjunctiva which is usually caused by infection or allergy. It is frequently referred to as pink eye and is the most common acute eye disorder seen by primary care pediatricians and family physicians.
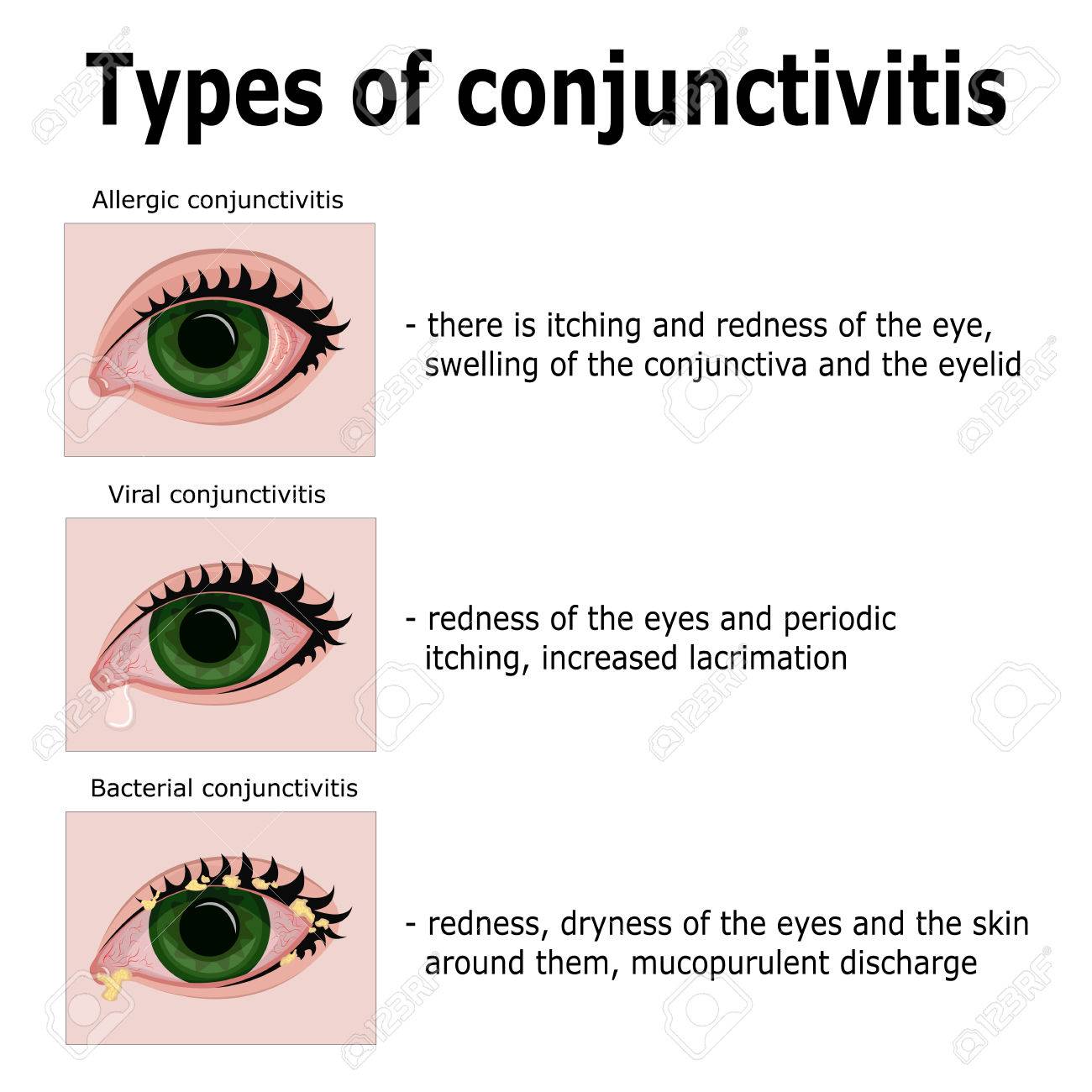
What are the characteristics of allergic conjunctivitis?
Allergic conjunctivitis is characterized by ocular redness and itching. Tearing (clear tears), crusting of the eye lids and photophobia may also be seen. The condition is often recurrent, and seasonal. Children who have allergic conjunctivitis often have a history of other atopic diseases, particularly allergic rhinitis, eczema or asthma.
What are the characteristics of an infectious conjunctivitis?
Infectious conjunctivitis may be bacterial or viral. Bacterial conjunctivitis is twice as common as viral conjunctivitis. Typically in bacterial conjunctivitis the eye is red, there is a purulent discharge, the affected child is often a pre-schooler and there may be an associated otitis media. In viral conjunctivitis there is redness, clear tearing or crusting, usually occurs in an older school age child, and is often associated with pharyngitis.
What organisms are commonly involved in bacterial conjunctivitis?
The most common bacterial organisms causing conjunctivitis are Haemophilus Influenzae and Streptococcus pneumoniae. H. Influenzae conjunctivitis occurs in 40 to 50% of cases and is more likely to be associated with an accompanying otitis media than other organisms. S. Pneumoniae accounts for about 10% of cases and other organisms (Staphylococcus aureus, Bacteroides and Moraxella catarrhalis) account for the remainder.
What is the most common cause of viral conjunctivitis?
Adenovirus conjunctivitis is the most common cause of viral conjunctivitis and may account for up to 20% of infectious conjunctivitis. Outbreaks of adenoviral conjunctivitis have been linked to contaminated equipment in ophthalmology clinics and to swimming pools.
Why is there a need to distinguish viral from bacterial conjunctivitis?
Viral and other non-purulent types of conjunctivitis do not require antimicrobial treatment. Often these children are treated mistakenly for prolonged periods of time with both topical and systemic antibiotics with persistence of the red eye. In some situations the topical antibiotic itself may cause an allergic reaction resulting in a persistent red eye.
What is the pathogenesis of infectious conjunctivitis?
In children the joint communication of the conjunctival sac with the middle ear and nasopharynx probably accounts for the frequent association of otitis media and pharyngitis with acute conjunctivitis.
What is the differential diagnosis of acute conjunctivitis?
In the child with a non-purulent conjunctivitis, one should think of Kawasaki disease, Lyme disease, juvenile rheumatoid arthritis orSteven's Johnson syndrome. When there is decreased vision and light sensitivity the physician must think of uveitis. Trauma and allergic conjunctivitis account for the remainder of the differential diagnosis.
What is the treatment of choice for acute bacterial conjunctivitis?
Acute bacterial conjunctivitis is a self limited condition. However, the use of antibiotic treatment is recommended because it hastens healing considerably and it eradicates the bacterial pathogen allowing children to return to daycare centers and schools within 24 hours of treatment. Topical treatment with polymyxin-bacitracin, garamycin or other suitable topical antimicrobials should be used. There is usually no need to use topical treatment for more than 2 to 5 days when complete resolution should have occurred. Treatment should be applied to both eyes, even if only one eye appears to be infected. Topical application should be applied four times a day.
What approach should be used if the purulent discharge persists despite topical treatment?
If there is persistent eye discharge after Day 4 or 5 of treatment then one needs to consider an alternative diagnosis. The most common occurrence is that of an associated otitis media which has not been recognized or has subsequently developed and requires the use of an oral systemic antibiotic. This occurs most frequently in H. influenzae conjunctivitis. An oral antibiotic which has activity against beta lactamase producing organisms should be used.
Conjunctivitis In Children - Kids Health NZ
What is the treatment for viral conjunctivitis?
Non-purulent viral conjunctivitis requires no treatment.
What is the treatment for allergic conjunctivitis?
Allergic conjunctivitis can be treated with an ophthalmic preparation containing a topical decongestant with or without antihistamine. Prevention of allergic conjunctivitis in susceptible individuals is best treated with topical sodium chromoglycate.[3]
Infectious conjunctivitis is highly contagious, soteach kids to wash their hands well and often with warm water and soap. They also should not share eye drops, tissues, eye makeup, washcloths, towels, or pillowcases.
Be sure to wash your own hands well after touching an infected child’s eyes, and throw away items like gauze or cotton balls after they’ve been used. Wash towels and other linens that the child has used in hot water separately from the rest of the family’s laundry to avoid contamination.
If you know your child is prone to allergic conjunctivitis, keep windows and doors closed on days when the pollen is heavy, and dust and vacuum often to limit allergy triggers. Irritant conjunctivitis can only be prevented by avoiding the irritating causes.
Screening and treating pregnant women for STDs can prevent many cases of pinkeye in newborns. A pregnant woman may have bacteria in her birth canal even if she shows no symptoms, which is why prenatal screening is important.
Conjunctivitis is a common eye condition that affects children, especially under 5 years of age. It can either be caused by an infection or by an allergy. Infectious conjunctivitis is contagious and may spread to other household members. Allergic conjunctivitis is more common in children with allergies such as hay fever.
Neonatal conjunctivitis and dacryocystitis
If your child has conjunctivitis, they may have:
a red or pink eye (or both eyes)
redness behind the eyelid
swelling of the eyelids, making them appear puffy
excessive tears
a yellow-green discharge from the eye which dries when your child sleeps, causing crusting around the eyelids
a gritty feeling (like there is sand in the eye)
itchiness of the eyes and eye rubbing
children with allergic conjunctivitis almost always rub their eyes excessively. They may also have an itchy or runny nose and sneezing
Your child does not need to be excluded from school or childcare if they have conjunctivitis.[8]
You need to contact a doctor or nurse today.
If your child has any of the following:
+ Severe pain in eyes
+ Extreme sensitivity to light (photophobia)
+ Changes in vision including flashing lights (vision can appear blurred or misted because of discharge smeared over the surface of the eye, but this will usually clear on blinking or wiping the eyes)
+ If you notice any redness, swelling or puffiness around the eye or eyelids.
+ Severe headache
+ Persistent vomiting
+ Blisters develop on the skin next to the eye
+ Babies under 28 days with a red eye(s) or lots of pus from their eye(s) - note although a sticky eye due to a blocked tear duct is a very common condition in babies (and does not require medical review), this condition does not cause a red eye
+ Is finding it hard to breathe
+ Seems dehydrated (sunken eyes, drowsy or not passed urine for 12 hours)
+ Is becoming drowsy (excessively sleepy) or irritable (unable to settle them with toys, TV, food or picking up) - especially if they remain drowsy or irritable despite their fever coming down
+ Has extreme shivering or complains of muscle pain
+ Is 1-3 months of age with a temperature of 38°C / 100.4°F or above, or 3-6 months of age with a temperature of 39°C / 102.2°F or above (but fever is common in babies up to 2 days after they receive vaccinations)
+ Continues to have a fever of 38.0°C or above for more than 5 days
+ Is getting worse or if you are worried bacterial conjunctivitis does not improve after 24 hours of antibiotic use
You need urgent help.If your child has any of the following:
- Becomes pale, mottled and feels abnormally cold to touch
- Is going blue around the lips
- Too breathless to talk / eat or drink
- Has a fit/seizure
- Becomes extremely agitated (crying inconsolably despite distraction), confused or very lethargic (difficult to wake)
- Develops a rash that does not disappear with pressure (see the 'Glass Test')
- Is under 1 month of age with a temperature of 38°C / 100.4°F or above
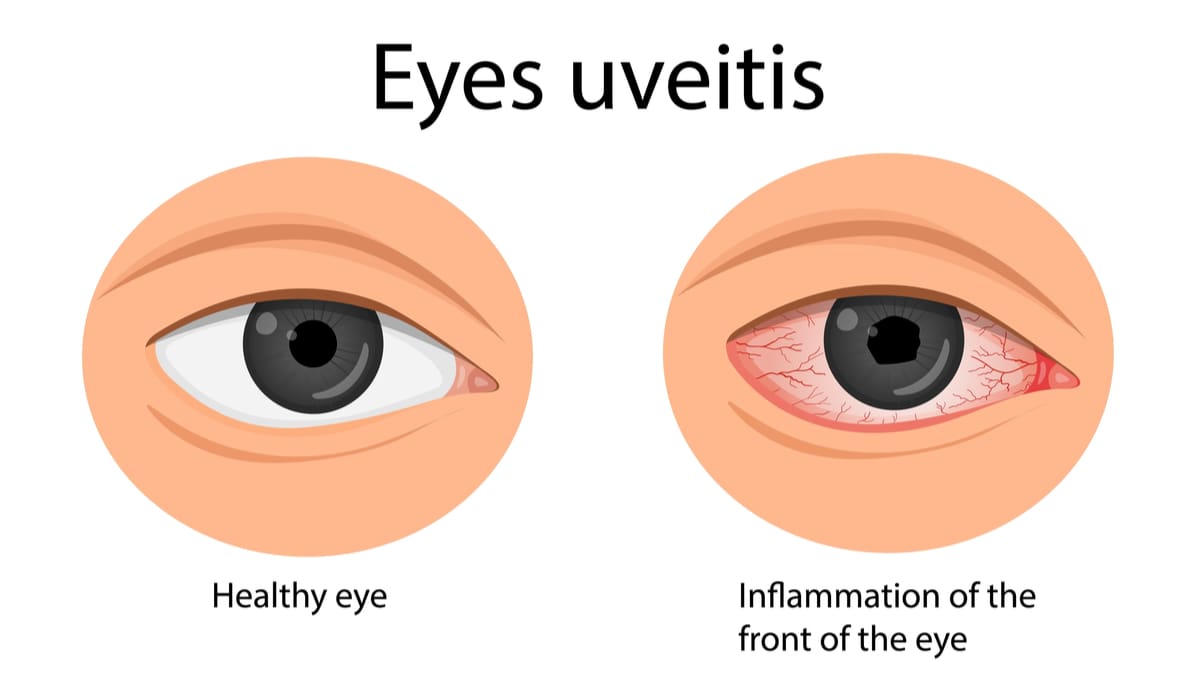
یوئیت(Uveitis)به التهاب بافت يووهآ(uvea) چشم گویند. يووهآ لایهٔ میانی چشم است و شامل عنبیه، جسم مژگانی و مشیمیه میباشد. بسیاری از انواع یووئیت مزمن هستند.
uvea /ˈjuːvɪə/
the pigmented layer of the eye, lying beneath the sclera and cornea, and comprising the iris, choroid, and ciliary body.[5]
علائم یوئیت:
علائم یووئیت عبارتند از:
تاري ديد
حساسيت به نور
ريزش اشك از چشم
اجسام شناور در ميدان بينايي
درد و قرمزي (قرمزي دور قرنيه)
البته علائم یوئیت بستگي به محل درگيري التهاب در سيستم يووهآ دارد.
اهميت يووهآ(uvea)چيست؟
بيشتر عروق خوني تغذيه كننده چشم در يووهآ ميباشد. التهاب يووهآ ميتواند بر قرنيه, شبكيه, صلبيه و قسمتهاي حياتي ديگر چشم تأثير گذارد. از آنجايي كه يووهآ در مجاورت بسياري از قسمتهاي مهم چشم قرار دارد لذا التهاب اين لايه از چشم ممكن است ديد را تهديد نموده و از التهابهاي شايعتر لايههاي بيروني چشم شديدتر باشد.
یوئیت قدامی Anterior : به التهاب عنبیه به تنهایی و یا به التهاب عنبیه و جسم مژگانی یوئیت قدامی اطلاق میشود.
یوئیت میانی Intermediate : به التهاب جسم مژگانی یوئیت میانی گفته میشود.
یوئیت خلفی Posterior : به التهاب مشیمیه گفته میشود. یوئیت میانی و یوئیت خلفی معمولاً بدون درد هستند. نشانههای یوئیت خلفی و یوئیت میانی شامل، کاهش دید و مگس پران (دیدن سایهای متحرک شبیه مگس در میدان بینایی) بوده و معمولاً دو طرفهاست. بیشتر بیماران دچار یوئیت میانی، در سنین طفولیت یا جوانی مبتلا میشوند.
یوئیت منتشر Panuveitis : به التهاب در همهٔ قسمتهای یوه یوئیت منتشرگفته میشود. یوئیت قدامی شایعترین نوع یووئیت است. نشانههای یوئیت قدامی ممکن است تنها در یک چشم بروز کند. بیمار ممکن است درد خفیف تا شدید، قرمزی چشم و حساسیت به نور داشته باشد. ممکن است دید بیمار نیز دچار کاهش شده باشد.
بیماری یووئیت منتشر مجموعهای از نشانههای همهٔ انواع را دارد.
علل يوئيت بسيار گوناگون است از جمله:
ويروس (مانند شينگل، مامپس يا هرپس)
قارچ(مانند هيستوپلاسموزيس)
پارازيت (مانند توكسوپلاسموزيس)
ممكن است باعث ايجاد يوئيت شوند. در بسياري از موارد علت ابتلا به بیماری یوئیت ناشناخته است. همچنين يووئيت ممكن است در نتيجه آسيب به چشم يا ناشي از بيماري باشد كه در نقاط ديگر بدن رخ داده است (مانند آرتريت). ايجاد التهاب در يك چشم ممكن است در نتيجه آسيب شديد چشم ديگر باشد(يووئيت همدرد Sympalhetic).
عوارض بیماری یوئیت چشم:
ممکن است بیماری یووئیت منجر به برخی عوارض از جمله آب مروارید، کاهش یا افزایش فشار چشم، آب سیاه، مشکلات شبکیه و کراتوپاتی باند شکل (Band keratopathy) شود. هر یک از این عوارض ممکن است منجر به کاهش دید شود. بیماری یوئیت چشم ممکن است در هر سنی بروز کند.
چگونگی تشخیص بیماری یوئیت چشم:
انجام معاينه دقيق چشم توسط چشم پزشك به هنگام بروز علائم از اهميت ويژهاي برخوردار است. التهاب درون چشمي ممكن است براي هميشه روي بينايي اثر بگذارد يا گاهي به نابينايي منجر شود. چشم پزشك از وسايل ويژهاي استفاده كرده، درون چشم را معاينه ميكند و غالباً بر همان اساس تشخيص بيماري را ميدهد.
در برخي شرايط انجام آزمايشهاي خوني، آزمايشهاي پوستي عكس از سينه و گاهي حتي نمونهبرداري به طريقه جراحي از چشم ممكن است در تشخيص مفيد باشند از آنجايي كه بیماری یوئیت ميتواند با وجود بيماري در قسمت هاي ديگر بدن همراه باشد، لذا ارزيابي و درك سلامتي عمومي بيمار حائز اهميت است. اين كار ممكن است نيازمند انجام مشاوره با متخصصين پزشكي ديگر باشد.
بیماری يوؤيت جدى است كه مى تواند عوارض دائمى روى چشم بگذارد، بنابراين بايد بلا فاصله بعد از تشخيص، درمان بیماری یوئیت چشم را شروع شود.
معمولا استروئيد (كورتون) به شكل قطره به همراه قطره سيكلوپلژيك مثل تروپيكاميد جهت كاهش درد و التهاب تجويز ميشود. بسته به نوع و شدت بيماري ممكن است استروئيد به صورت تزريق اطراف چشم ويا قرص خوراكى نيز تجويز گردد. یوئیت قدامي بدليل گرفتاري قسمت هاي قدامي چشم، معمولا با قطره قابل درمان است.
گاهي در درمان یوئیت از داروهاي ديگري كه باعث كنترل التهاب مي شوند و اصطلاحا به آنها ايمونوساپرسيو (سرکوبگر سیستم ایمنی) گفته مي شود، استفاده مي گردد. اين داروها و همچنين استروئيدها ممكن است عوارضي ايجاد كنند كه شامل گلوكوم، كاتاراكت، افزايش قند خون، افزايش فشار خون، مشكلات كليوي و پوكي استخوان مي باشند.
بنابراين بسيار مهم است كه فردی که دارای بیماری یوئیت است دستورات دارويي پزشك را بدقت اجرا کند و بيمار بطور منظم تحت معاينه و پيگيري قرار گيرد، تا پيشرفت بيماري و يا عوارض ناشي از داروهای یوئیت تحت كنترل باشد. گاهي در يوئيت هاي مزمني كه لازم است سالها دارو مصرف كنند، دارو را به صورت مخازني در داخل چشم كاشته، و دارو به مدت چند ماه يا سال بتدريج در داخل چشم آزاد مي گردد.[4,5]
Uveitis (pronounced you-vee-EYE-tis) is basically an inflammation of the eye. The condition involves all inflammatory processes of the middle layers of the eye, also called the uveal tract or uvea. The uvea includes the iris (colored part of the eye), choroid (a thin membrane containing many blood vessels) and ciliary body (the part of the eye that joins these together).
The uvea is very important because its many veins and arteries transport blood to the parts of the eye that are critical for vision.
Symptoms of uveitis may include: eResearch by Navid Ajamin -- summer 2011
Eye redness and irritation
Blurred vision
Eye pain
Increased sensitivity to light[1]
Floating spots before the eyes
Alteration of the color of the iris
Photophobia - abnormal sensitivity to light
Eye redness
General vision problems
Floaters - debris in the eye make you see tiny rods, chains of transparent bubbles floating around in your field of vision
Cloudy vision
Headaches
A small pupil[3]
Uveitis may develop rapidly, and it is very important that you see your ophthalmologist for a complete eye exam if you develop these symptoms, especially if a painful, red eye does not clear up quickly.Left untreated, uveitis may permanently damage your vision.[1]
About half of all uveitis cases — with most occurring in the anterior uvea — don't have an obvious cause. Symptoms of anterior uveitis include light sensitivity, decreased visual acuity and eye pain.
Intermediate and posterior uveitis usually are painless. Symptoms of these types of uveitis include blurred vision and floaters, typically in both eyes. Most people who develop intermediate uveitis are in their teens, 20s or 30s.
Diffuse uveitis has a combination of symptoms of all types of uveitis.[2]
Uveitis has many potential causes, including infection with a virus, fungus, bacteria or parasite, inflammatory disease affecting other parts of the body, or injury to the eye.
There are four types of uveitis:
Iritisis the most common form of uveitis. It affects the iris and is often associated with autoimmune disorders such as rheumatoid arthritis. Iritis may develop suddenly and may last up to eight weeks, even with treatment.
Cyclitisis an inflammation of the middle portion of the eye and may affect the muscle that focuses the lens. This also may develop suddenly and last several months.
Retinitisaffects the back of the eye. It may be rapidly progressive, making it difficult to treat. Retinitis may be caused by viruses such as shingles or herpes and bacterial infections such as syphilis or toxoplasmosis.
Choroiditisis an inflammation of the layer beneath the retina. It may also be caused by an infection such as tuberculosis.
Because uveitis is serious, treatment needs to begin right away. For uveitis not caused by an infection, your ophthalmologist may prescribe eye drops containing steroids to reduce swelling and drugs to relieve pain. Antibiotics are used in patients with infectious uveitis.
Dark glasses will help with light sensitivity.
Complications of uveitis may include glaucoma, cataracts,abnormal growth of blood vessels in the eyes that interfere with vision, fluid within the retina, and vision loss. Early diagnosis and treatment by your ophthalmologist is critical.[1]
New evidence shows that smoking also appears linked to development of uveitis, according to a study reported in the March 2010 issue of Ophthalmology.
"Cigarette smoke includes compounds that stimulate inflammation within the blood vessels, and this may contribute to immune system disruption and uveitis," said University of California San Francisco (UCSF) researcher and ophthalmologist Dr. Nisha Acharya.[2]
Types of Uveitis
There are four types of uveitis: anterior, intermediate, posterior and panuveitis.
Anterior uveitis (also called iritis) affects the front section of the uvea, including, the tissue between the iris and the cornea, the iris itself, and the ciliary body. This type is usually the easiest to treat.
Intermediate uveitis affects the middle of the uvea, including the retina, the blood vessels behind the lens and the vitreous (the transparent, gel-like substance in the center of the eye).
Posterior uveitis affects the back of the uvea, including the retina or the choroid (the tissues that make up the wall in the back of the eye. This type is difficult to treat and is most likely to cause severe complications.
Panuveitis affects all three layers of the uvea at once. This is the rarest type of uveitis.[6]
What are the risk factors of uveitis? [7]
Patients over 60, those with long-term uveitis, and some who have uveitis in the middle or back of the eye might be at increased risk of complications. If left untreated, uveitis can cause long-term problems such as:
Cataracts, which cloud the lens of the eye
Damage to the optic nerve that can lead to vision loss
Detachment of the retina
Glaucoma, when fluid can’t drain from the eye leading to increased pressure in the eye
Macular edema, or swelling of the retina
Retina scarring in spots, which can lead to vision loss
Permanent vision loss
Reference:
medicinenet.com
allaboutvision.com
medicalnewstoday.com
lod.ir
dictionary.com
myvision.org/eye-conditions/uveitis
utswmed.org/medblog/uveitis-eye-inflammation
nicetoview.blogfa.com
وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.
















 وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.
وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.