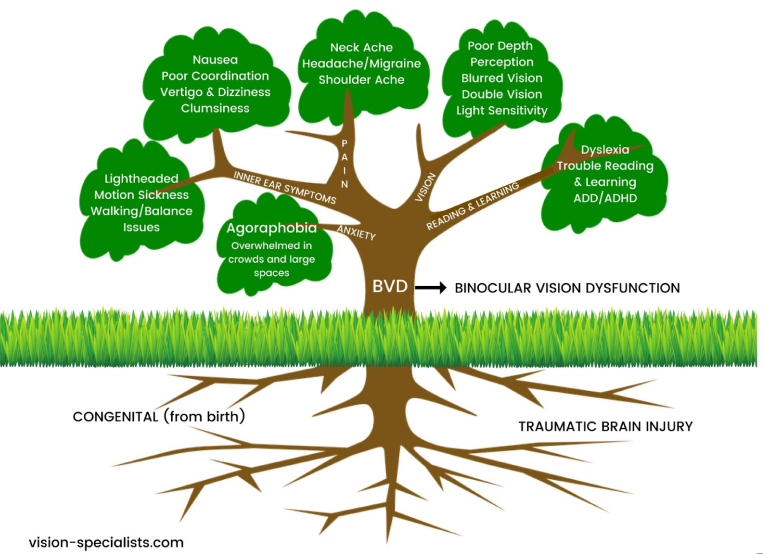
BVD(Binocular vision dysfunction) and other binocular vision issues can have a huge impact on your life, both at work and at home, which is why it’s so important to understand what BVD is and the signs and symptoms to watch for.

In order for the eyes to work together as a team, they must be in perfect alignment. When they’re not, a number of unpleasant and sometimes painful physical symptoms can occur. Headaches, dizziness and balance issues are some of the most common indicators that BVD is present.
Other signs include:
- Reading problems (losing your place frequently, skipping lines), as well difficulty comprehending what was read.
- Severe light sensitivity and blurred/shadowed/doubled vision.
- Anxiety and apprehension when in large, open indoor spaces with tall ceilings.
Treatment can include any of the following:
- Custom micro-prism lenses that help realign the eyes, thus greatly reducing or even eliminating the symptoms of BVD.
- Prism contact lenses that treat BVD, as well as contact lenses for astigmatism.[8]
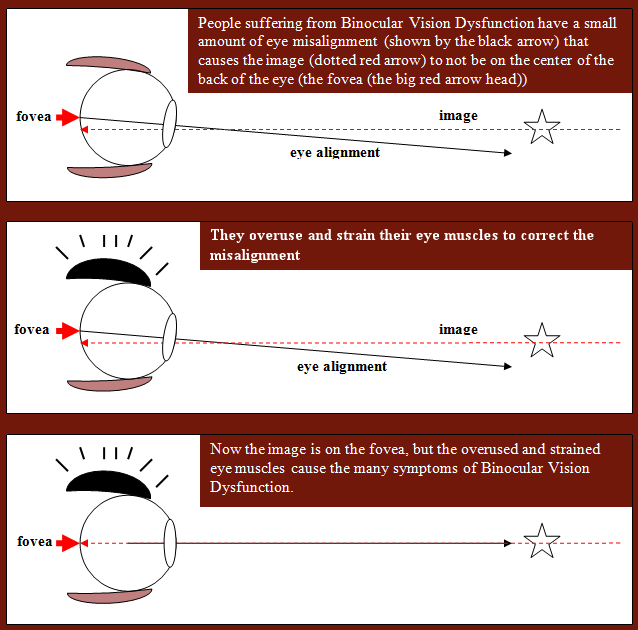
Binocular vision dysfunction (BVD) is a visual condition where the line of sight from one eye tends to be slightly out of alignment with the line of sight from the other eye (usually vertical) and this puts heavy strain on the eye muscles as they are constantly trying to correct the alignment to achieve single focus vision.
The cause can be secondary to: normal facial asymmetry, acquired facial asymmetry from aging or head trauma from sports or injury damaging the nerves to your eye muscles causing the imbalance.


Binocular vision dysfunction means you see two images that compete in the middle where their fields of view overlap.
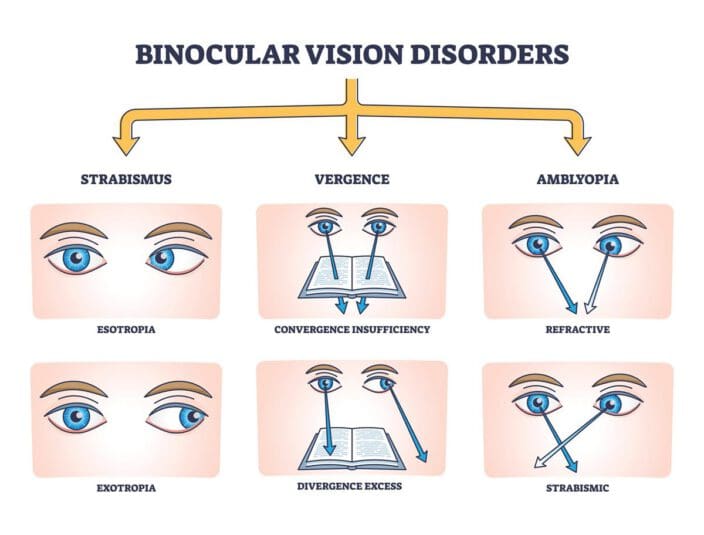
There are three forms of BVD:
1. Vertical Heterophoria
2. Superior Oblique Palsy
3. Horizontal misalignment
Symptoms of BVD
Those who suffer from Vertical Heterophoria or Superior Oblique Palsy tend to have a small amount of vertical eye misalignment, which the brain corrects by directing the eye muscles to properly reposition the eyes. However, using the eye muscles in this manner overworks them and they become strained and fatigued, causing the many symptoms of Vertical Heterophoria and Superior Oblique Palsy:
- Anxiety in crowds or large open spaces
- Overly sensitive to light and glare
- Double vision
- Shadowed, overlapping or blurred vision
- Skip lines or lose your place while reading.
- Quickly fatigue while reading and difficulty with comprehension.
- Closing or covering one eye to make it easier to see.
- Headaches
- Dizziness
- Lightheadedness
- Nausea
- Anxiety
- Motion sickness
- Poor depth perception
- Lack of good balance and drifting while walking
- Poor coordination and Clumsiness
- Aching eyes, especially with eye movement
- Neck, upper back or shoulder pain
- Head tilting [2]
There are a number of tests the doctor may perform to assess any difficulties with vision, including:
Developmental Eye Movement (DEM): Reading eye movements and assessing their accuracy.
Sensory Fusion Assessment: This is a series of four separate examinations to discover if suppression, which can be part of an overall binocular vision disorder, is present.
Near Point of Convergence (NPC): The test will find out if convergence and divergence dysfunctions are causing problems.
Accommodative Convergence/Accommodation (AC/A): Any evidence of accommodation which exists is discovered by the results of this test. [4]
Binocular vision is vision in which creatures having two eyes use them together. The word binocular comes from two Latin roots, bini for double, and oculus for eye. According to Fahle (1987), having two eyes confers six advantages over having one.

- It gives a creature a spare eye in case one is damaged.
- It gives a wider field of view. For example, humans have a maximum horizontal field of view of approximately 190 degrees with two eyes, approximately 120 degrees of which makes up the binocular field of view (seen by both eyes) flanked by two uniocular fields (seen by only one eye) of approximately 40 degrees.
- It can give stereopsis in which binocular disparity (or parallax) provided by the two eyes' different positions on the head gives precise depth perception. This also allows a creature to break the camouflage of another creature.
- It allows the angles of the eyes' lines of sight, relative to each other (vergence), and those lines relative to a particular object (gaze angle) to be determined from the images in the two eyes.These properties are necessary for the third advantage.
- It allows a creature to see more of, or all of, an object behind an obstacle. This advantage was pointed out by Leonardo da Vinci, who noted that a vertical column closer to the eyes than an object at which a creature is looking might block some of the object from the left eye but that part of the object might be visible to the right eye.
- It gives binocular summation in which the ability to detect faint objects is enhanced.

Once the fields of view overlap, there is a potential for confusion between the left and right eye's image of the same object.
This can be dealt with in two ways:
- one image can be suppressed, so that only the other is seen,
- or the two images can be fused.
If two images of a single object are seen, this is known as double vision or diplopia.
Fusion of images (commonly referred to as 'binocular fusion') occurs only in a small volume of visual space around where the eyes are fixating. Running through the fixation point in the horizontal plane is a curved line for which objects there fall on corresponding retinal points in the two eyes. This line is called the empirical horizontal horopter. There is also an empirical vertical horopter, which is effectively tilted away from the eyes above the fixation point and towards the eyes below the fixation point. The horizontal and vertical horopters mark the centre of the volume of singleness of vision. Within this thin, curved volume, objects nearer and farther than the horopters are seen as single. The volume is known as Panum's fusional area (it's presumably called an area because it was measured by Panum only in the horizontal plane). Outside of Panum's fusional area (volume), double vision occurs. eResearch by Navid Ajamin -- spring 2016

When very different images are shown to the same retinal regions of the two eyes, perception settles on one for a few moments, then the other, then the first, and so on, for as long as one cares to look.
This alternation of perception between the images of the two eyes is called binocular rivalry.
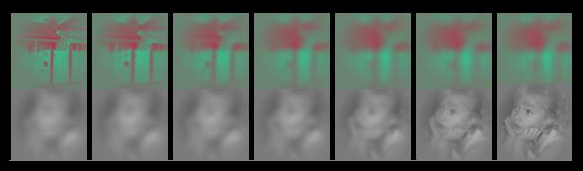
When different images are shown to the two eyes, awareness can alternate such that each is intermittently suppressed and only one image is seen at a time. For instance, a picture of a girl can be shown to the left eye and a picture of a house to the right. Perception can then alternate - swapping between seeing the girl and the house. This phenomenon is called Binocular Rivalry.
 Binocular Rivalry has generated broad interest as it permits an opportunity to explore the relationship between changes in conscious vision and brain activity in the absence of changes to sensory input. However, the function of binocular suppression remains a point of contention.[7]
Binocular Rivalry has generated broad interest as it permits an opportunity to explore the relationship between changes in conscious vision and brain activity in the absence of changes to sensory input. However, the function of binocular suppression remains a point of contention.[7]
Binocular rivalry is a phenomenon of visual perception in which perception alternates between different images presented to each eye.
Humans have limited capacity to process an image fully at one time. That is why the binocular rivalry occurs. Several factors can influence the duration of gaze on one of the two images. These factors include context, increasing of contrast, motion, spatial frequency, and inverted images. Recent studies have even shown that facial expressions can cause longer attention to a particular image. When an emotional facial expression is presented to one eye, and a neutral expression is presented to the other eye, the emotional face dominates the neutral face and even causes the neutral face to not been seen.
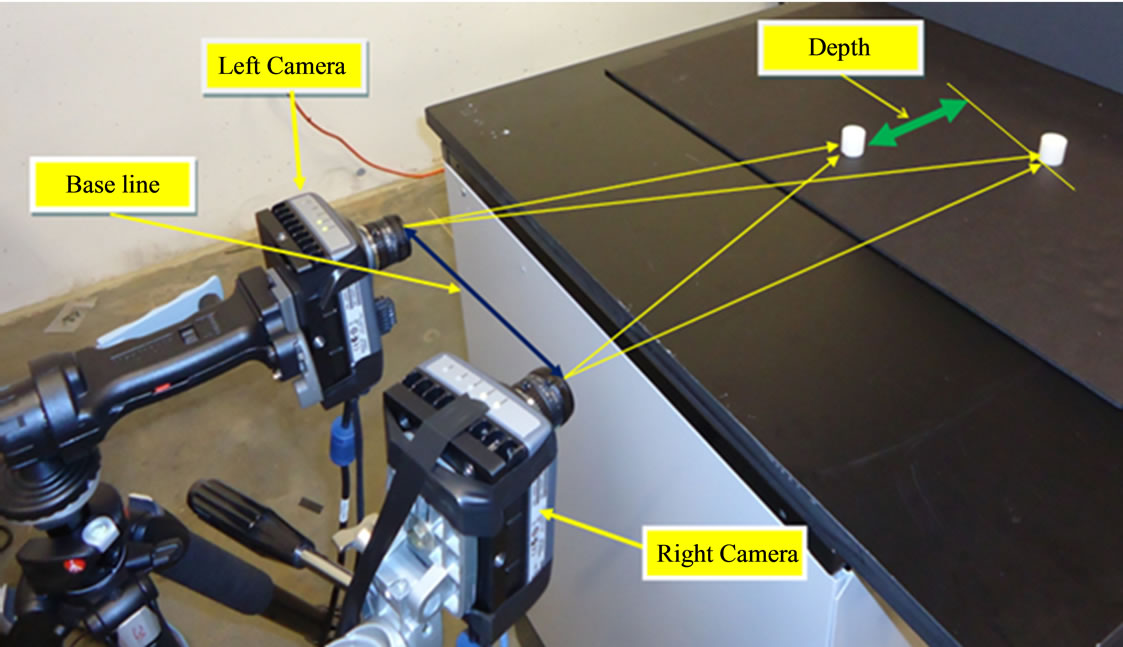
Binocular depth perception arises as a consequence of the slightly displaced point of view of the two eyes. The horizontal displacement of image features in the two eyes (i.e. binocular disparities) makes it possible to reconstruct the depth relationships in the visual world.
The term depth perception refers to our ability to determine distances between objects and see the world in three dimensions. To do this accurately, one must have binocular stereoscopic vision, or stereopsis.
Depth perception is the ability to judge depth and distance. Depth perception requires binocular vision, but it may be assisted by monocular cues such as motion parallax, or how objects move in relation to the movement of the head; interposition, or object overlap; and color and contrast cues that suggest distance.
What causes depth perception problems?
There is not one answer, but in fact several conditions that can contribute to poor depth perception:
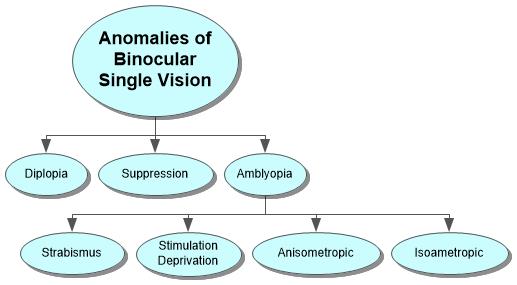
- Strabismus – This is a condition where both of the eyes cannot be aligned simultaneously. One or both eyes may turn outwards, inwards, downwards, or upwards. This is commonly referred to as being cross-eyed.
- Blurred vision – This is when one’s vision is not as sharp as normal and it makes it incredibly difficult to spot detail.
- Amblyopia – This is a condition where one eye cannot focus as well as the other and is often called a “lazy eye.”
- Eye trauma – Eye trauma is anything that disturbs or harms the eye. This prevents the eye or eyes from working as well as they should and can harm one’s vision.
 Not everyone sees optimally. People suffering from amblyopia, optic nerve hypoplasia and strabismus often have reduced depth perception. A person with an injury to one eye, or a person missing one eye, may not be able to tell where objects are in relation to others. Visual therapy may help improve these problems.
Not everyone sees optimally. People suffering from amblyopia, optic nerve hypoplasia and strabismus often have reduced depth perception. A person with an injury to one eye, or a person missing one eye, may not be able to tell where objects are in relation to others. Visual therapy may help improve these problems.
Depth perception plays an important part in many activities. Driving, sewing, threading a needle, watching 3D movies and even walking on uneven ground all require certain levels of depth acuity. People without functioning stereoscopic vision may not be able to perform these activities or may struggle with them.
Two-eyed, or binocular vision, allows each eye to see from different angles. The brain processes the information coming from each eye and forms it into one image—a process called convergence. If binocular vision is working as it should be, the brain can interpret the information, which is called stereopsis. Those that have vision in only one eye usually have to rely on other cues to aid their depth perception.
Binocular matching of local features in the retinal images may be used to obtain estimates of the absolute disparity (and distance) of objects or surfaces, as well as the relative disparity (or relative distances) between different objects.

Other phenomena of binocular vision include:
- utrocular discrimination (the ability to tell which of two eyes has been stimulated by light),
- eye dominance (the habit of using one eye when aiming something, even if both eyes are open),
- allelotropia (the averaging of the visual direction of objects viewed by each eye when both eyes are open),
- binocular fusion or singleness of vision (seeing one object with both eyes despite each eye's having its own image of the object),and
- binocular rivalry (seeing one eye's image alternating randomly with the other when each eye views images that are so different they cannot be fused).
When different images are presented to the two eyes, they compete for perceptual dominance, such that one image is visible while the other is suppressed. This binocular rivalry is thought to reflect competition between monocular neurons within the primary visual cortex. However, neurons whose activity correlates with perception during rivalry are found mainly in higher cortical areas, and respond to input from both eyes. Thus rivalry may involve competition between alternative perceptual interpretations at a higher level of analysis. To investigate this, we tested the effect of rapidly alternating the rival stimuli between the two eyes. Under these conditions, the perceptual alternations exhibit the same temporal dynamics as with static patterns, and a single phase of perceptual dominance can span multiple alternations of the stimuli. Thus neural representations of the two stimuli compete for visual awareness independently of the eye through which they reach the higher visual areas. This finding places binocular rivalry in the general category of multistable phenomena, such as ambiguous figures, and provides a new way to study the neural cause and resolution of perceptual ambiguities.

Binocular vision helps with performance skills such as catching, grasping, and locomotion.It also allows humans to walk over and around obstacles at greater speed and with more assurance.Orthoptists are eyecare professionals who fix binocular vision problems.[1]
Strabismus occurs when there are neurological or anatomical problems that interfere with the control and function of the extraocular muscles. The problem may originate in the muscles themselves, or in the nerves or vision centers in the brain that control binocular vision.
Grades of binocular vision
There are grades and methods of assessing binocular vision. The grades are the different steps in the development of stereopsis during the visual maturation. Testing of the grades is done by a synaptophore and graded as - no binocular single vision grade zero, simultaneous perception grade 1, fusion grade 2 and stereopsis grade 3. Limited form of testing can be done with worth four-dot test or Bagolini’s glasses.
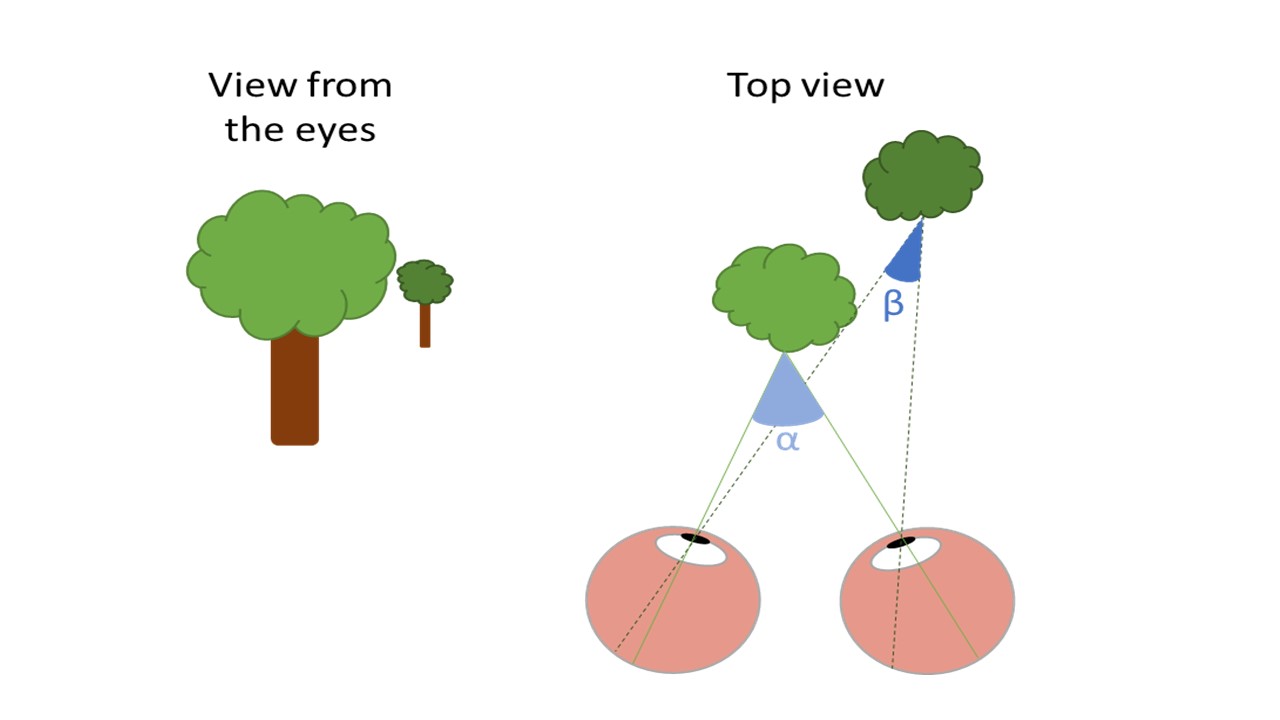 The drawing at the left shows the view of two trees from the perspective of the eyes. The light green tree stands in front of the dark green tree. The right drawing shows a top view of the scene. When the eyes are focusing on the light tree, the image is projected on the fovea of the left and right eye. The angle between both projections is angle α. The images of the dark tree are projected on different positions of the peripheral retina in the left and right eye with angle ß. Because angle ß is smaller than angle α our brain interprets the dark tree as further away than the light tree. The size of the difference between α and ß represents the disparity. Large differences in angle indicate large differences in depth
The drawing at the left shows the view of two trees from the perspective of the eyes. The light green tree stands in front of the dark green tree. The right drawing shows a top view of the scene. When the eyes are focusing on the light tree, the image is projected on the fovea of the left and right eye. The angle between both projections is angle α. The images of the dark tree are projected on different positions of the peripheral retina in the left and right eye with angle ß. Because angle ß is smaller than angle α our brain interprets the dark tree as further away than the light tree. The size of the difference between α and ß represents the disparity. Large differences in angle indicate large differences in depth
Stereopsis is not present at birth but develops in the first months of life. That full-term and pre-term children develop stereopsis at the same age post-birth shows that the development depends on visual experience rather than biological maturation of the system.In the early months of life, we develop coarse stereopsis, which operates on high contrast lines and edges and enables us to align our eyes.
Four basic types of Da Vinci stereopsis cues
Alignment then permits the development of fusion and fine stereopsis. Fine stereopsis works over a much shorter range of disparities but enables us to make very fine depth judgments even in densely textured surfaces, such as grass or tree bark, where there are few or no depth cues monocularly.
important binocular visual skills:
- Tracking: the ability to move the eyes across a sheet of paper
- Fusion: the ability to use both eyes together at the same time
- Stereopis: binocular depth perception
- Convergence: the ability of the eyes to move and work as a team
- Visual Motor Integration: the ability to transform images from a vertical to a horizontal plane [3]

Reference:
- en.wikipedia.org/wiki/Binocular_vision
- city-optometry.com
- children-special-needs.org
- rebuildyourvision.com
- intechopen.com/books/visual-cortex-current-status-and-perspectives/...
- deskarati.com/2014/03/10/binocular-rivalry
- psy.uq.edu.au/~uqdarnol/Rivalry.htm
- vision-specialists.com/articles/the-causes-symptoms-of-binocular-vision-dysfunction-your-questions-answered
- shopfelixgray.com/blog/understanding-depth-perception
- nearsay.com/c/670447/515154/a-guide-to-depth-perception
- eyehealthweb.com/depth-perception
- wisegeek.com/what-is-depth-perception.htm
- ncbi.nlm.nih.gov/m/pubmed/8602261
- eyewiki.aao.org/Stereopsis_and_tests_for_stereopsis
- opticianonline.net/cet-archive/4723
- allaboutvision.com/conditions/strabismus.htm
See also:
- BINOCULAR VISION webeye.ophth.uiowa.edu Department of Ophthalmology & Visual Sciences
- Binocular Vision Dysfunction (BVD) -- dizziness-and-balance.com




















































 وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.
وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.