Oculomotor apraxia (OMA) is the absence or defect of controlled, voluntary, and purposeful eye movement. It was first described in 1952 by the American ophthalmologist David Glendenning Cogan.
People with this condition have difficulty moving their eyes horizontally and moving them quickly. The main difficulty is in saccade initiation, but there is also impaired cancellation of the vestibulo-ocular reflex. Patients have to turn their head in order to compensate for the lack of eye movement initiation in order to follow an object or see objects in their peripheral vision, but they often exceed their target. There is controversy regarding whether OMA should be considered an apraxia, since apraxia is the inability to perform a learned or skilled motor action to command, and saccade initiation is neither a learned nor a skilled action.[1]
Causes
OMA is a neurological condition. Although some brain imaging studies of people with OMA reveal a normal brain, some MRI studies have revealed unusual appearance of some brain areas, in particular the corpus callosum, cerebellum, and fourth ventricle. Oculomotor apraxia can be acquired or congenital. Sometimes no cause is found, in which case it is described as idiopathic.
A person may be born with the parts of the brain for eye movement control not working, or may manifest poor eye movement control in childhood. If any part of the brain that controls eye movement becomes damaged, then OMA may develop. One of the potential causes is bifrontal hemorrhages. In this case, OMA is associated with bilateral lesions of the frontal eye fields (FEF), located in the caudal middle frontal gyrus. The FEF control voluntary eye movements, including saccades, smooth pursuit and vergence. OMA can also be associated with bilateral hemorrhages in the parietal eye fields (PEF).
The PEF surround the posterior, medial segment of the intraparietal sulcus. They have a role in reflexive saccades, and send information to the FEF. Since the FEF and PEF have complementary roles in voluntary and reflexive production of saccades, respectively, and they get inputs from different areas of the brain, only bilateral lesions to both the FEF and PEF will cause persistent OMA. Patients with either bilateral FEF or bilateral PEF damage (but not both FEF and PEF) have been shown to regain at least some voluntary saccadic initiation some time after their hemorrhages. Other causes of OMA include brain tumors and cardiovascular problems.[1] eResearch by Navid Ajamin -- winter 2025
The source of OMA is in the central nervous system (brain). The process of initiating eye movements is a complicated neural pathway involving many different structures. Imaging of the brain with magnetic resonance imaging (MRI) is commonly performed when evaluating OMA. Findings may be normal or may reveal poor development of regions of the brain, in particular: the corpus callosum, cerebellum, and/or fourth ventricle. OMA can be an isolated condition, genetic, or associated with other syndromes.
Idiopathic congenital OMA is referred to as Cogan-type and is often associated with developmental delay. Risk factors include gestational and perinatal problems.
Cases have been reported in older individuals after lesions in parts of the brain.
Associated conditons. OMA has been described in a wide range of clinical entities, including metabolic and neurodegenerative conditions. A few examples include: ataxia with oculomotor apraxia, ataxia-telangiectasia, vitamin E deficiency, Gaucher’s disease, and Joubert syndrome.[2]
Symptoms[5]
Along with difficulties associated with eye movement, children may also experience low muscle tone, learning difficulties, and delays in language development. Delay in sitting, walking, and toilet training has also been observed.
Since some infants with ISID do not appear to visually follow a moving huge object, they are initially misdiagnosed as blind. Horizontal head thrusts become apparent as head control develops, usually around 4–6 months of age. In typically developing children, the frequency of head movements decreases as they get older during gaze transitions.
Early-onset OMA, along with infantile muscular hypotonia, early-onset ataxia, and newborn respiratory problems, is a common sign of Joubert syndrome (JBTS). There is also evidence of episodic tachypnea and apnea, as well as developmental delay and intellectual disabilities.
Vertical saccade involvement, nystagmus, and developmental abnormalities are linked to non-idiopathic OMA. Endocrine abnormalities may also be more common in OMA children than in the overall pediatric population.
What is Joubert syndrome(JBTS)? [4]
Joubert syndrome (JS) is a recessive disorder that is characterized by midbrain-hindbrain malformation and shows the “molar tooth sign” on magnetic resonance imaging.
Joubert syndrome is a rare genetic disorder that happens when the part of a fetus's brain doesn't develop as it should. The syndrome has many subtypes that cause different symptoms, but it typically causes issues with muscle control or muscle tone, breathing and eye movement.
Joubert syndrome causes different conditions and may change as children grow up. Symptoms may include physical differences, including facial differences, symptoms of certain eye conditions, and liver and kidney disease.
Your child may have the following neurological issues or conditions:
Hypotonia (decreased muscle tone) that becomes ataxia (issues with muscle coordination).
Eye conditions like nystagmus or strabismus (crossed eyes).
Breathing issues like tachypnea (fast, shallow breathing) or apnea (breathing that pauses).
Developmental delay.
Intellectual disability.
unable to initiate eye movements
The patient is unable to initiate eye movements Inability to saccade and pursue freely When you want to look to the right, you turn your head right to compensate. When you want to look to the left, you compensate by turning your head left.
Some patients have defects in only one direction, left or right.
Some patients have problems with both left and right directions.
You know what the sun can do to skin, right? Many a parent has learned the hard way. A few carefree hours in the sun – without sunscreen – can wreak havoc on the tender skin of children.
Well, their eyes are just as delicate. But while many parents religiously slather on the sunscreen, very few are just as careful with their kids’ eyes.
So, if you’re ready to go out and buy your kids sunglasses, read on to find out what to look for, and what to avoid. [1]
Sources of UV The main source of UVR is sunlight. Artificial lighting contributes to a lesser extent but may increase with the advent of energy efficient light sources.
Ambient UV: direct radiation, scatter, and reflection Direct sunlight only partly contributes to ambient UV. Under average conditions, more than 50% of ocular exposure comes from scattering and reflection from clouds and the ground.
The World Health Organisation’s solar ultraviolet index (UVI), an international index of UV burden assesses risk of UV damage to the skin. Several studies have shown that this is not a valid indicator of eye protection and potentially misleading.
Identifying absorption and transmission of UVR within structures of the eye is key to understanding potential damage.
UV transmission is strongly dependant on age. Below 9 years of age, a larger portion (2-5%) of UVA is transmitted by the cornea and the lens. Significant inter-individual differences have also been shown.
Acute and chronic damage to the eye by UV and visible light has been extensively studied, including epidemiological studies, with greater significance on chronic exposure.
Cornea The cornea is most exposed, with the greatest level of UVR absorption from direct irradiation. In addition oblique rays are reflected across the cornea and anterior chamber into the limbal area leading to elevated pathologies in this area. Most common diseases: Pterygium, pinguecula, climatic droplet keratopathy.
Cortical cataract It is known that UV light induces cataracts with a damage threshold at 350 nm of 60 mJ/cm2. With growing and aging populations and other changing demographic factors the incidence and prevalence of cataracts will increase. Reducing the risks that can lead to cataracts is therefore important.
Dry eye, premature presbyopia, AMD Decreasing tear film production linked to ageing, reduces UV absorption and antioxidant production by tears.
The association between UVR and AMD remains controversial. Blue light is a more significant contributor to development of AMD.
UV related skin aging and diseases of periorbital skin The acute response of the skin to UV is inflammation (sunburn). Clinical symptoms include erythema, swelling, pain and pruritus.
Chronic effects includephotoaging and photocarcinogenesis. Some clinical signs of photoaged skin include dryness, irregular pigmentation, lentigines, wrinkling and inelasticity. The delicate periorbital skin is particularly susceptible to effects of photoaging.
Mitochondrial DNAis a chromophore for UVA and UVB and subject to damage by UVR. DNA deletions are increased by up to 10-fold in photoaged skin compared to sun-protected skin of the same individual.
Photocarcinogenesis includes the development of actinic keratosis, squamous cell carcinoma, basal cell carcinoma, and malignant melanoma. 5% to 10% of skin cancers are appearing on the eyelids.
SPF measures sunscreen protection from UVB rays, the kind that cause sunburn and contribute to skin cancer. SPF does not measure how well a sunscreen will protect from UVA rays, which are also damaging and dangerous. Dermatologists recommend using a SPF15 or SPF30 sunscreen.
Higher SPFs don't give much more protection.[2]
SPF is an abbreviation for "sun protection factor." A sunscreen's protection factor (SPF) is figured by comparing how long it takes sunscreen-protected skin to burn to the length of time it takes unprotected skin to burn. The higher the SPF, the more protection you get against UVB rays.[3]
Sunglasses should be the first thing we reach for after applying sunscreen then, maybe a hat. With concerns over possible thinning of the ozone layer, the need to protect our bodies from UV exposure is becoming a growing concern.
It's more than a concern over sunburn. Our eyes as well as our skin need protection from UVA and UVB rays. These harmful invisible light rays are implicated as one of the leading causes of cataracts andmacular degeneration. Children are of particular concern and should wear sunglasses for their protection as sun damage is cumulative with most ill effects occurring before age 25. Even on cloudy days, UV rays can be just as damaging to the eyes. Don’t save sunglasses for only the brightest days. Wear them when spending any time outdoors. eResearch by Navid Ajamin -- spring 2016
Quality ophthalmic sunglasses will give 100% protection against UVA and UVB. There are different types of ophthalmic lenses one should consider when purchasing sunglasses. Glass lenses are more scratch resistant but they are heavier and can shatter if hit with an object. Plastic lenses are lighter and available in more colors and coatings. Polycarbonate lenses offer the most protection from breaking and are recommended for sports and should be considered for active children.[4]
skin around our eyes is ten times thinner than the skin on our face and Sunscreens are not tested to be used around eye area ,So it is better not to use sunscreens for around the eyes.
The heat can be very harsh on your eyewear specifically if you have a plastic frame. What ever you do, remember not to leave your sunglasses in the car! If it’s nearing 100 degrees outside your car, it’s probably approaching 200 inside the car.
Excessive heat can cause your prescription lenses to peel or permanently smudge your anti-reflective coating. This is true even for the more durable forms of anti-reflective coating like Kodak brand Clean & Clear.
The heat can cause your plastic sunglass frame to actually warp, essentially melting the plastic. Now this does not look like some bad B-rated horror movie where your glasses literally liquify, usually it makes the frame flatten out and get wider. This of course produces some fitting problems for the wearer as the glasses will then be consistently falling off.
Take extra care of your eyewear in the harsh summer heat. Keep yourself (and your glasses) cool!
Choose a sunscreen labelled broad spectrum or high protection against UVA and UVB so it offers balanced UVA and UVB protection.
Do not stay in the sun too long, even whilst using sunscreen, as no sunscreen can provide 100% protection.
Use a high protection sunscreen and re-apply frequently and generously, especially after perspiring, swimming or towelling.
In sunny weather, seek shade between 11am and 3pm when UV is at its strongest.
Cover up with clothing and don’t forget to wear a hat that protects your face, neck and ears, and weargood quality UV protective sunglasses.
Never let your skin burn and remember, a tan is a sign of sun damage to the skin.
Children have more sensitive skin and need extra care – use sunscreen, clothing and shade. Keep babies and young children out of direct sunlight.
We protectour skin with sunscreen, but what about our eyes?
Most of us are aware of the dangerous effects ultraviolet (UV) rays have on our skin, but few of us realize the danger imposed on our eyes.
UV radiation, whether from natural sunlight or artificial UV rays, can damage the eye's surface tissues as well as the cornea and lens. UV radiation can burn the front surface of the eye, much like a sunburn on the skin.
UV radiation consists of invisible rays from the sun.
There are three types of UV radiation: UVA, UVB and UVC.
UVC rays do not pose any threat, as they are absorbed by the ozone layer. However, exposure to UVA and UVB rays can have adverse effects on your eyes and vision. Short- and long-term exposure to these dangerous rays can cause significant damage damage. It is important to note that UV radiation can also be given off by artificial sources like welding machines, tanning beds and lasers.
Two types of harmful light rays come from the sun:
ultraviolet A radiation (UVA), and ultraviolet B radiation (UVB).
UVA radiation can cause photoaging, or premature aging of the skin, resulting in wrinkles, uneven pigmentation, and texture changes.
UVB radiation is the main cause of sunburn.
Short-Term Effects of UV Radiation
If you are exposed, unprotected, to excessive amounts of UV radiation over a short period of time, you are likely to experience an effect called photokeratitis. Photokeratitis is an inflammation of the cornea caused by a brief exposure to UV radiation, usually when combined with cold wind and snow. Like a "sunburn of the eye", it may be painful and may create symptoms includingred eyes, a foreign body sensation or gritty feeling in the eyes, extreme sensitivity to light and excessive tearing. Fortunately, this is usually temporary and rarely causes permanent damage to the eyes.
Long-Term Effects of UV Radiation
Long-term exposure to UV radiation can be more serious. Scientific studies and research growing out of the U.S. space program have shown that exposure to small amounts of UV radiation over a period of many years may increase the chance of developing a cataract, and may cause damage to the retina, the nerve-rich lining of the eye that is used for seeing. This damage to the retina is usually not reversible. Cumulative damage of repeated exposure may contribute to chronic eye disease, as well as increase the risk of developing skin cancer around the eyelids. Long-term exposure to UV light is also a risk factor in the development ofpterygium (a growth that invades the corner of the eyes) and pinguecula (a yellowish, slightly raised lesion that forms on the surface tissue of the white part of your eye.)
UV Radiation Protection
It is not yet known how much exposure to UV radiation will cause how much damage, but a good recommendation is to wear quality sunglasses that offer good protection and a wide-brimmed hat when working outdoors, participating in outdoor sports, taking a walk, running errands or doing anything in the sun.
To provide protection for your eyes, your sunglasses should:
block out 99 to 100 percent of bothUV-A and UV-B radiation
screen out 75 to 90 percent of visible light
be perfectly matched in color and free of distortion and imperfection
have lenses that are gray for proper color recognition
If you spend a lot of time in bright sunlight, wrap-around frames can provide additional protection from harmful UV radiation by keeping UV rays from reaching the eyes. Also, remember UV eye protection forchildren and teenagers. eResearch by Navid Ajamin -- summer 2013
They typically spend more time in the sun than adults. Finally,even if you are wearing contact lenses that have UV protection, you still need to wearsunglasses.UV rays will likely affect the eye tissue that is not covered by the contacts. Your eyes will be more comfortable, too, with most of the bright light blocked.
Reference: Vision.about.com Source: American Optometric Association. U/V Protection. 14 Jun 2007.
Bifocal glasses are used to correct vision at two distances—a prescription on top for far away and a different prescription on the bottom for near. Most people think of bifocals as reading glasses for people over forty who lose their ability to focus up close as they age. But children can also need reading glasses.
Many children have not developed sufficient control over their focusing systems, the natural lens inside the eye that keeps images clear, especially up close. Some children lack the ability to sustain sufficient focusing over an extended time period, so after a while print begins to blur. Others can’t make fast focusing shifts from one distance to another, like from the board to their desks, so any time they look away, everything is blurry. Some children have a tendency to over focus, and the additional stress causes eyestrain and headaches. If they over focus too much, the additional tension on the visual system can make the eyes to turn too far inward, causing double vision. Finally, near work at school places much more stress on the visual system than distance viewing, and some young children respond by translating the visual stress into physical and emotional symptoms—back and neck tension, headaches, constriction of their perceptual fields and a reduction in their visual space, a tendency to develop nearsightedness, and avoidance of the reading tasks that are causing the physical and visual discomfort. eResearch by Navid Ajamin -- spring 2013
Prescribing reading glasses effectively treats many of these problems. A convex plus lens relaxes the child’s focusing system, relieving much of the visual stress. In fact, prescribing a low power plus lens is so effective in keeping children’s visual system comfortable during extended close work at school that they are often called “learning lenses.”
Reading glasses that use a bifocal are a good option for school-aged children who only need the additional correction up close. The bifocal gives them the lens support they need for deskwork but doesn’t change their distance vision. Sometimes vision therapy is also prescribed when the focusing problem is severe enough that additional interventions are also required.
New advances in lenses allow children flexibility in the type of bifocal they choose. Many children still prefer the flat-top bifocalbecause the line separating the two powers helps them tell exactly where their distance prescription ends and their near prescription starts. However, some children or parents don't like the look of the "line", so for them progressive no-line bifocals are a good option. The lens is made so that the change between prescriptions is so gradual no line appears. Another very popular option is the "half-moon" bifocal. It has the advantage of a clear delineation between powers liked lined bifocals but when the glasses are on the child's face, the bifocal is invisible like progressive lenses.
When bifocals or reading glasses are prescribed, it is important that children wear them for all close work, especially at school and during homework. Sometimes children will only need the bifocals for a few years as they develop control of their focusing system. Others may need the additional near-point support for as long as they are in school and spending a lot of time reading.Bifocals are an important tool for optometrists when working with children who spend up to eight hours a day using their eyes for reading and school work.
bifocal or varifocal for kids
Many children have not developed sufficient control over their focusing systems, the natural lens inside the eye that keeps images clear, especially up close. Some children lack the ability to sustain sufficient focusing over an extended time period, so after a while print begins to blur. Others can’t make fast focusing shifts from one distance to another, like from the board to their desks, so any time they look away, everything is blurry. Some children have a tendency to over focus, and the additional stress causes eyestrain and headaches. If they over focus too much, the additional tension on the visual system can make the eyes to turn too far inward, causing double vision. Finally, near work at school places much more stress on the visual system than distance viewing, and some young children respond by translating the visual stress into physical and emotional symptoms—back and neck tension, headaches, constriction of their perceptual fields and a reduction in their visual space, a tendency to develop nearsightedness, and avoidance of the reading tasks that are causing the physical and visual discomfort.
Prescribing reading glasses effectively treats many of these problems. A convex plus lens relaxes the child’s focusing system, relieving much of the visual stress. In fact, prescribing a low power plus lens is so effective in keeping children’s visual system comfortable during extended close work at school that they are often called “learning lenses.”
Reading glasses that use a bifocal are a good option for school-aged children who only need the additional correction up close. The bifocal gives them the lens support they need for deskwork but doesn’t change their distance vision. Sometimes vision therapy is also prescribed when the focusing problem is severe enough that additional interventions are also required.
New advances in lenses allow children flexibility in the type of bifocal they choose. Many children still prefer the flat-top bifocal because the line separating the two powers helps them tell exactly where their distance prescription ends and their near prescription starts. However, some children or parents don't like the look of the "line", so for them progressive no-line bifocals are a good option. The lens is made so that the change between prescriptions is so gradual no line appears. Another very popular option is the "half-moon" bifocal. It has the advantage of a clear delineation between powers liked lined bifocals but when the glasses are on the child's face, the bifocal is invisible like progressive lenses.
When bifocals or reading glasses are prescribed, it is important that children wear them for all close work, especially at school and during homework. Sometimes children will only need the bifocals for a few years as they develop control of their focusing system. Others may need the additional near-point support for as long as they are in school and spending a lot of time reading.
By adding an additional lens power for up close, optometrists are able to adjust children’s focusing system to give them better control and eliminate eyestrain, blurred vision, headaches, and fatigue.
Reference:
childrensvision.com Children's Vision Information Network
Convergence insufficiency occurs when your eyes don't turn inwardproperly while you're focusing on a nearby object. When you read or look at a close object, your eyes should converge — turn inward together to focus — so that they provide binocular vision and you see a single image. But if you have convergence insufficiency, you won't be able to move your eyes inward to focus normally.
Convergence insufficiency is caused by complications coronating eye movements and muscles. Instead of the eyes coming together (converging) to focus on objects close by, one or both eyes point outward. Because the brain controls all eye movement, damage to the brain is the leading cause of convergence insufficiency. However, the exact cause of this condition remains a mystery. The working theory among researchers is that neurogenerative disease such as Parkinson’s disease, myasthenia gravis and Alzheimer’s disease in some way cause CI.
Convergence insufficiency (CI) is a common eye condition that affects the ability of the eyes to work together. This condition occurs when the eyes are unable to converge or move inward effectively, making it difficult to focus on objects that are close up. This can cause a variety of symptoms, including eye strain, headaches, blurred vision, and difficulty reading.
Symptoms
Not everyone with convergence insufficiency experiences symptoms. Signs and symptoms occur while you're reading or doing other close work and may include:
Tired, sore or uncomfortable eyes (eyestrain)
Headaches
Blurred vision
Difficulty reading — words seem to float on the page, you lose your place or you read slowly
Double vision
Difficulty concentrating
A "pulling" feeling around your eyes
Sleepiness
Squinting, rubbing or closing one eye
Trouble concentrating. It can be difficult to focus and pay attention. In school, children may do work slowly or avoid reading, which can affect learning.
If you or your child experiences symptoms of convergence insufficiency or has problems reading, consult an eye care professional, such as an ophthalmologist or an optometrist. A technician called an orthoptist may assist the eye care professional in evaluating and treating convergence insufficiency.
Convergence insufficiency results from misalignment of the eyes when focusing on nearby objects. The exact cause isn't known, but the misalignment involves the muscles that move the eye. Typically, one eye drifts outward when you're focusing on a word or object at close range.
Complications
Difficulties with reading and concentrating can adversely affect a child's learning. Convergence insufficiency typically isn't detected in routine eye exams or school-based vision screenings. A child with the condition may be evaluated for learning disabilities because of his or her reading troubles.
Tests and diagnosis
People with convergence insufficiency may have otherwise normal or "20-20" vision, and the condition may not be detected during a routine eye exam. To diagnose convergence insufficiency, your eye doctor may do the following, including special eye-focusing tests:
Treatments and drugs
If convergence insufficiency isn't causing symptoms, you generally don't need treatment. But for people with symptoms, treatment with eye-focusing exercises can increase the eyes' convergence ability. Treatment may take place in the office of a trained therapist or at your home.
Treatments may include:
A study sponsored by the National Eye Institute of the National Institutes of Health compared home-based treatment with doctor office-based treatment for convergence insufficiency in children ages 9 to 17. Study results showed that the most effective therapy was a weekly hourlong session of in-office vision therapy with at-home reinforcement exercises. Other studies have also found that office-based treatment is effective about 75 percent of the time.
Home-based treatment with pencil pushups or computer programs hasn't been shown to be as effective — in some studies, it works only about one-third of the time. But home treatment costs less and is more convenient. Only a small percentage of eye care providers offer in-office therapy for convergence insufficiency. Many people who can't find or can't afford in-office therapy opt for home-based treatment.
If you choose home treatment, many experts recommend using computer software programs along with pencil pushups. The combined approach may be more effective, and the computer therapy is more engaging for children.
Treatment for convergence insufficiency may take three months or longer, though you'll likely start to see improvement in your symptoms after four weeks. After your convergence ability has improved, you can help maintain your improved vision by continuing to read and do other near tasks. Treatment can permanently cure convergence insufficiency, but symptoms may come back after an illness, lack of sleep or when you're doing a lot of reading or other close work. In rare cases, eye-focusing exercises don't work and your doctor may recommend surgery.
eResearch by Navid Ajamin -- spring 2013
Take a medical history. This may include questions about problems you have with focusing, blurred or double vision, headaches, and other signs and symptoms.
Vision Therapy for Convergence Insufficiency
Measure the near point of convergence (NPC). This test measures the distance from your eyes to where both eyes can focus without double vision. For this simple test, the examiner holds a small target, such as a glass ball, printed card or penlight, in front of you and slowly moves it closer to you until either you experience double vision or the examiner recognizes that your eyes can no longer focus together.
Assess positive fusional vergence (PFV). During this test, you're asked to read letters on an eye chart while looking through prism lenses. The examiner will note when you begin to have double vision.
Perform a routine eye exam. If you have any other vision problems, such as nearsightedness, your ophthalmologist or optometrist may conduct tests to assess the degree of the problem.
Pencil pushups. In this simple exercise, you focus on a small letter on the side of a pencil as you move it closer to the bridge of your nose, stopping the movement if you have double vision. The exercise is often done for 15 minutes a day, five or more days a week.
Computer vision therapy. Eye-focusing exercises are done on a computer using special software designed to improve convergence. You may print out the results to share with your eye doctor.
Reading glasses. Glasses with built-in prisms force your eyes to work harder to align and are sometimes used for people who need help with their reading vision. But they can be tiring to your eyes and generally haven't proved effective.
Your brain controls all your eye movements. When you look at a nearby object, your eyes move inward to focus on it. This coordinated movement is called convergence. It helps you do close work like reading or using a phone.
Convergence insufficiency is a problem with this movement. The condition causes one or both eyes to drift outward when you look at something close by.
Doctors don’t know what causes convergence insufficiency. However, it’s associated with conditions that affect the brain.
These may include:
traumatic brain injury
concussion
Parkinson’s disease
Alzheimer’s disease
Graves’ disease
myasthenia gravis
Convergence insufficiency appears to run in families. If you have a relative with convergence insufficiency, you’re more likely to have it, too.
Your risk is also higher if you use the computer for long periods of time. Diagnosing convergence insufficiency
It’s common for convergence insufficiency to go undiagnosed. That’s because you can have normal vision with the condition, so you can pass a normal eye chart exam. Plus, school-based eye exams aren’t enough to diagnose convergence insufficiency in children.
You’ll need a comprehensive eye exam instead. An ophthalmologist, optometrist, or orthoptist can diagnose convergence insufficiency.
Visit one of these doctors if you are experiencing reading or visual problems. Your child should also see an eye doctor if they’re struggling with schoolwork.
At your appointment, your doctor will do different tests.
They might:
Ask about your medical history. This helps your doctor understand your symptoms. Perform a full eye exam. Your doctor will check how your eyes move separately and together. Measure near point of convergence. Near point convergence is the distance you can use both eyes without seeing double. To measure it, your doctor will slowly move a penlight or printed card toward your nose until you see double or an eye moves outward. Determine positive fusional vergence. You’ll look through a prism lens and read letters on a chart. Your doctor will note when you see double.
Vision Exams
Following symptom analysis, a comprehensive vision exam is vital. These exams are not just about checking visual acuity; they involve a series of tests specifically designed to evaluate the eyes’ ability to converge when focusing on close objects. Key tests include:
Cover Test: Determines how the eyes move and work together.
Near Point of Convergence (NPC): Measures the closest point at which the eyes can focus together without double vision.
Positive Fusional Vergence (PFV) at Near: Assesses the ability to sustain focus on a close target without experiencing double vision or discomfort.
Usually this question is asked when the children are pre-verbal or if they can’t quite yet read the eye chart. A lot of parents mistakenly think that there is no way to figure out if the infant or toddler needs glasses and that just isn’t true. As parents, there are a couple signs and symptoms you can look out for which may indicate that your child is having difficulty seeing. These might not always mean that your child needs glasses.
Sometimes, certain things can be habit (squinting or tilting the head) or sometimes they can mean your child needs glasses or has a more serious eye problem.
The American Academy of Pediatrics and American Academy of Ophthalmology recommends that all children have their vision checked at the 4 year old visit at the pediatrician’s office. If your child is premature, has other medical problems, or you have noticed abnormalities, the child can be checked earlier.
If your child is struggling at school, an undetected vision problem may be to blame. A child who is unable to see the blackboard clearly or has a hard time focusing on the work at his desk will soon become frustrated. Many children’s vision problems go undetected during school vision screenings, so parents and teachers should watch for the following signs that may signal vision problems.
If you notice any of these signs in your child, schedule an appointment for a full eye exam. The doctor may determine that your child is nearsighted or farsighted, vision problems that are easily corrected.
1. Squinting
Squinting is much like looking through a pinhole. Peeking through a small opening reduces the size of the blurred image on the back of the retina. This temporarily improves vision and could be a sign of your child compensating for poor vision.
2. Tilting the head
Tilting the head can be a sign of an eye muscle imbalance or strabismus. A child may have double vision when looking down or in a certain direction. Tilting the head may minimize the double vision to a more manageable level.
3. Sitting too close to the television Sitting very close to the television or lowering the head while reading is often a sign of nearsightedness. Nearsighted people generally have clear vision at a close range and poor vision at a distance. Moving closer to an object brings the object to their clear focal point and makes the image larger.
4. Losing place while reading
Skipping lines or losing your place while reading can be a sign of a vision problem. Often,astigmatism or an eye muscle problem such as strabismus is to blame.
5. Covering one eye to read or watch television
A child who covers one eye to read is simply shutting the eye with the poorer vision off so that it does not interfere with their vision. An uncorrected vision problem in one eye can increase a child's risk of developing amblyopia. Covering one eye can also be a sign of double vision caused by strabismus or a more serious medical problem, such as a cataract.
6. Excessive tearing
Children often have lag ophthalmus, a condition which causes the eyes to dry out at night because the eyelids do not completely close while sleeping. This can cause excessive tearing during the day that interferes with good vision.
7. Rubbing eyes Rubbing the eyes is a sign of eye fatigue and can be a sign of all types of vision problems. Medical conditions such as allergic conjunctivitis can also cause vision problems.
8. Finger pointing while reading
Finger pointing while reading is not always a bad sign. It is often seen in a child learning to read independently. However, it can be sign of an uncorrected vision problem such as amblyopia. Amblyopic eyes exhibit a ‘crowding’ phenomenon. When letters or words appear very close to other letters or words, it makes them difficult to recognize.
9. Light sensitivity
Children with exotropia, a type of strabismus, occasionally squint one eye when exposed to bright sunlight. This may be interpreted as light sensitivity.
10. Frequent headacheseResearch by Navid Ajamin -- spring 2013 Uncorrected farsighted children often have frontal headaches or brow aches. This is a result of the child attempting to compensate by exerting extra effort to clear their blurry vision.
What to Do If Your Child Fails a Vision Screening
Normally, vision screenings are conducted by your child’s pediatrician or school. “If your child fails a vision screening, the most import thing to do is be seen by an eye care provider for a comprehensive eye exam,” Collins says.
A comprehensive exam assesses visual acuity, or the clarity and sharpness of vision, and may also check for:
Strabismus (crossed eyes) and eye alignment
Depth perception
Overall health of the inside and outside of the eye
Indications of more serious eye conditions
If your child already has glasses, it’s important to get eyes checked by an eye care provider every year.
Optimal vision is essential to the learning process. Many people don’t realize how many problems poor vision can cause for school-aged children. Therefore, it is important to be aware of your child’s overall eye health and what you can do to safeguard it.
ورم ملتحمه نوزادیبا علائم قرمزی ، اشک ریزش ، ترشح چشم ، التهاب ملتحمه و پلک زخم و حتی با سوراخ شدن قرنیه مشخص می شود .
چشم صورتی یا التهاب ملتحمه یک التهاب با علل و عوامل ایجادکنندهٔ مختلف در ملتحمهٔ چشمهاست. در این مطلب میتوانید با التهاب ملتحمهٔ چشم در کودکان، علل، عوامل، انواع و درمان آن آشنا شوید.
Neonatal conjunctivitis, also called ophthalmia neonatorum, typically presents during the first four weeks of life. The infection is usually acquired during delivery and is the most common ocular disease in neonates. Typical symptoms are persistent tearing and a mucoid discharge in the inner corner of the eye.
Is newborn eye discharge normal?
It is normal for a baby to have sticky yellow or white discharge in the corner of one or both eyes and can cause the eyelashes to stick together. This can last for several months.
What is the difference between dacryocystitis and conjunctivitis?
Conjunctivitis is characterized by redness, itching, and discharge from the eye. While it shares the symptom of discharge with dacryocystitis, conjunctivitis typically involves more diffuse redness across the conjunctiva and lacks the localized swelling over the lacrimal sac evident in dacryocystitis.
P39.1
ICD-10 code P39. 1 for Neonatal conjunctivitis and dacryocystitis is a medical classification as listed by WHO under the range - Certain conditions originating in the perinatal period .
Is bacterial pink eye spreadable?
Pink eye caused by viruses and bacteria can easily spread from person to person in different ways. You can get pink eye from: Close personal contact, such as touching or shaking hands. Contact with droplets from the air after an infected coughs or sneezes.
Pneumococcal conjunctivitis is a bacterial eye infection that causes symptoms such as redness, discharge, and crusting of the eyelids. It is caused by a type of bacterium called Streptococcus pneumoniae. Streptococcus pneumoniae can cause many other types of infections, including middle ear infections and sinusitis.[9]
Chlamydia trachomatis is an obligate intracellular parasite and has been identified as the most common infectious cause of neonatal conjunctivitis. The reservoir of the organism is the maternal cervix or urethra.
? Is pink eye contagious
التهاب ملتحمه در کودک
التهاب ملتحمه که کنژنکتیویت و چشم صورتی نیز نامیده میشود، یک التهاب بسیار شایع و قابل درمان ملتحمهٔ چشم یعنی غشای شفافی هست که درون پلکها و سفیدی چشمها را پوشانده است. عروق خونی هنگامی که ملتهب میشوند، مشهودتر میشوند و ویژگی مشخصهٔ این عارضه را که صورتی یا قرمز شدن چشم است ایجاد میکنند. التهاب میتواند توسط عفونت، یک مادهٔ آلرژیزا یا دیگر عوامل محرک ایجاد شود. همچنین التهاب ملتحمهٔ ناشی از عفونتهای باکتریایی و ویروسی بسیار مسری هستند.
علائم التهاب ملتحمه در کودک
اگر سفیدی یک یا هر دو چشم کودکتان و لبهٔ پایین هر کدام از پلکهایش قرمز باشد، احتمال دارد که التهاب ملتحمه داشته باشد. در حینی که سیستم ایمنی بدن کودک برای مبارزه با عفونت تلاش میکند، ممکن است چشمانش اشکریزی داشته باشند، چسبنده شوند یا شوره بزنند. به محض اینکه متوجه علائم التهاب ملتحمه شدید، با پزشک کودک تماس بگیرید.
به خاطر داشته باشید مهم است که فوراً درمان آن را شروع کنید، تا از گسترش ویروسها جلوگیری کنید و از عارضهٔ ثانویهٔ نادر عفونت پلک و بافت نرم دور چشم پیشگیری شود. قرمزی خفیف چشمها و کمی ورم پلک در یک نوزاد ممکن است نوع کوتاهمدتی از التهاب ملتحمه باشد که در واکنش به قطرههای چشمی ایجاد میشود که در هنگام تولد به نوزادان میدهند.
دلایل و عوامل التهاب ملتحمه در کودک
Patient education: Conjunctivitis (pink eye)
التهاب ملتحمهٔ چشم دلایل مختلفی دارد که برخی از چند دلیل محتملتر آن میتواند شامل موارد زیر باشد: ویروس: اگر کودک شما مبتلا به التهاب ملتحمه و همچنین علائم سرماخوردگی است، عفونت به احتمال زیاد ویروسی است. ویروسها شایعترین عامل ایجاد التهاب ملتحمه هستند. باکتری: اگر چشمهای کودکتان ترشحات زرد غلیظی ایجاد میکنند که باعث ورم پلکها یا چسبیدن آنها به یکدیگر میشود، احتمالاً علت آن باکتریهایی مانند استافیلوکوکها، استرپتوکوکها یا هموفیلوسها است. همچنین نوعی جدی از التهاب ملتحمه باکتریایی به نام افتالمیا نئوناتوروم وجود دارد که در نوزادانی که در طول زایمان مادرشان در معرض کلامیدیا یا سوزاک قرار گرفتهاند بروز میکند. آلرژن: واکنشهای آلرژیک در کودکان زیر یک سال نادر است، اما اگر چشمهای کودکتان خارشدار و متورم و دچار آبریزش و خونگرفتگی هستند و یا آبریزش بینی نیز دارد، ممکن است واکنشی آلرژیک به یک عامل محرک مانند گرد و غبار، گرده یا دود باشد. قطرههای چشمی نوزاد: قطرهٔ چشمی که در هنگام تولد برای جلوگیری از عفونت باکتریایی به نوزاد داده میشود میتواند چشمهایش را تحریک کنند. این عارضه گاهی اوقات کنژنکتیویت شیمیایی نامیده میشود. مجاری اشکی مسدود: حداقل ۲۰ درصد از نوزادان در حالی متولد میشوند که یک یا هر دو مجرای اشکی آنها به طور کامل یا جزئی مسدود شدهاند. این انسداد میتواند منجر به علائمی شبیه التهاب ملتحمه مانند ترشحات سفید یا زرد یا یک التهاب ملتحمه تمامعیار شود. عوامل دیگر: هر چیزی که بتواند چشم و پوشش داخلی پلکها را تحریک کند، از مه یا دود، گرفته تا کلر موجود در استخر شنا میتواند باعث ایجاد این التهاب شود. eResearch by Navid Ajamin -- spring 2012
درمان التهاب ملتحمه در کودک
اگر نوزادتان التهاب ملتحمه دارد، بلافاصله با پزشک خود تماس بگیرید. التهاب ملتحمه میتواند برای یک نوزاد عفونتی جدی باشد. پزشک چشمهای کودک را معاینه خواهد کرد و در مورد علائمش سؤال میکند. هرچند درمان با نوع التهاب ارتباط دارد ولی بسیاری از پزشکان توصیه میکنند که برای کمک به پاک کردن هر نوع ترشحاتی در همهٔ انواع التهاب ملتحمه و درمان هر گونه عفونت اولیه یا حتی جلوگیری از عفونت، چند قطره از شیر دوشیدهشدهٔ مادر را چندین بار در روز در چشمهای آسیبدیده بریزید. درمان هر یک از انواع التهاب ملتحمه به شکل زیر است:
التهاب ملتحمهٔ ویروسی: التهاب ملتحمهٔ ویروسی توسط انواعی از ویروسها ایجاد میشود. این نوع کنژنکتیویت معمولاً طی یک هفته یا همین حدود بهبود مییابد. برای درمان نیز پزشک به شما توصیه خواهد کرد که ناحیهٔ درگیر را با شستن چشمهای کودک با آب گرم و پاک کردن ترشحات خشکشده تمیز کنید و لازم است این کار را با ملایمت انجام دهید. اگر چشمهای کودک پس از دو هفته بهبود نیافت، دوباره پزشک را در جریان بگذارید.
گذاشتن کمپرس گرم روی چشم هم ممکن است تسکیندهنده باشد. برای این کار کافی است یک پارچهٔ تمیز را در آب گرم خیس کنید و آن را روی چشمهای کودک خود قرار دهید، برای مثال وقتی در حال شیر خورن است.
التهاب ملتحمهٔ باکتریایی: اگر باکتری عامل بروز التهاب ملتحمه باشد، پزشک پماد یا قطرهٔ آنتیبیوتیکی را تجویز میکند تا برای حدود هفت روز به چشمهای کودکتان اعمال کنید. زدن پماد ممکن است برایتان راحتتر از قطرههای چشمی باشد. برای زدن پماد ابتدا دستهایتان را بشویید و سپس به آرامی پلک پایین کودک را اندکی پایین بکشید و یک خط از پماد را در امتداد آن بمالید. وقتی تیوب را فشار میدهید و کودک چشمهایش را باز و بسته کند، پماد وارد چشمهایش میشود.
اگر هم از قطرهٔ آنتیبیوتیک استفاده میکنید، آن را در گوشهٔ چشم کودکتان بریزید. انجام این کار در زمانی که چشم او بسته است سادهتر خواهد بود. هنگامی که کودک چشمش را باز میکند، دارو وارد چشمش میشود. دستهای خود را قبل و بعد از ریختن دارو در چشمهای کودکتان بشویید. هرگز از داروهای او برای شخص دیگری استفاده نکنید و از قطرهها یا پمادهای قدیمی استفاده نکنید. داروهای قدیمی به احتمال زیاد استریل نیستند و میتوانند عفونت را بدتر کنند.
اطمینان حاصل کنید که کودکتان دورهٔ کامل آنتیبیوتیکهای تجویزشده را حتی بعد از اینکه علائمش از بین رفتهاند، مصرف میکند. در غیر این صورت ممکن است عفونت برگردد. پزشک احتمالاً توصیه میکند چشمهای کودک خود را با آب گرم شستوشو دهید و ترشحات خشکشده را با ملایمت بردارید، زیرا تجمع مایعات عفونی میتواند از اثرگذاری آنتیبیوتیکها بکاهد. گذاشتن کمپرس گرم روی چشم ممکن است تسکیندهنده باشد. یک پارچهٔ تمیز را در آب گرم خیس کنید و آن را روی چشمهای کودک خود قرار دهید، برای مثال در حینی که شیر میخورد.
التهاب ملتحمهٔ آلرژیک: راهحل مقابله با این نوع التهاب این است که مادهٔ آلرژیزا را شناسایی کنید و کودک خود را دور از آن نگه دارید. میتوانید در مورد روشهای مقابله با آلرژی کودک خود را بخوانید. اگر چشمهای کودک او را اذیت میکند، یک کمپرس سرد ممکن است به تسکین التهاب ملتحمهٔ آلرژیک کمک کند.
التهاب ملتحمهٔ شیمیایی: این واکنش به قطرههای چشمی نوزاد است که برای جلوگیری از عفونت به او داده میشود و احتمالاً در حدود ۲۴ تا ۳۶ ساعت طول میکشد.
همچنین به خاطر داشته باشید که التهاب ملتحمهٔ باکتریایی و ویروسی هر دو فوقالعاده مسری هستند. بنابراین، برای جلوگیری از گسترش عفونت، هر بار که مراقبتهای چشم کودک را انجام میدهید، دستهای خود را بشویید. حولهها، لباسها و ملافههای کودک خود را از دیگران جدا کنید و آنها را مرتب بشویید.
شروع ورم ملتحمه می تواند از چند ساعت تا چند هفته بعد از تولد شروع شود .
Pink Eye in Kids: What Every Parent Needs to Know
عوامل ایجاد کننده ورم ملتحمه عوامل باکتریایی یا ویروسی مانند : گونوگوکی ، استاف اورئوس ، کلامیدیا ، هموفیلوس آنفلوآنزا ، پسودوموناس ، استرپتوکوک ، پنوموکوک ، هرپس سیمپلکس می باشند.
در میان این علل سه عامل مهم تر وخطرناک تر است : ورم ملتحمه گونوکوکی ، ورم ملتحمه کلامیدیائی ، ورم ملتحمه با ویروس هرپس سیمپلکس تیپ 2
ورم ملتحمه گونوگوکی :
1-4 روز بعد از تولد شروع می شود و با ترشحات چرکی فراوان ، ورم ملتحمه و تورم پلک ها خود را نشان می دهد از عوارض وخیم وفاجعه آمیز آن زخم وسوراخ شدن قرنیه و و عفونت داخل چشم ( آندوفتالمیت) است . که می تواند به سرعت باعث کوری شود
انواع ورم ملتحمه میکروبی با درمان آنتی بیوتیک قابل درمان است.
ورم ملتحمه کلامیدیائی :
که معمولا 1-2 هفته بعد از تولد شروع می شود با ترشحات چرکی والتهاب ملتحمه و با شدت کمتراز نوع گونوکوکی تظاهر می کند همانند گونوکوک در اثر آلوده شدن چشم نوزاد در هنگام عبور از کانال زایمانی ایجاد می شود و یکی از علل شایع ورم ملتحمه نوزادی است .
جهت پیشگیری از ورم ملتحمه نوزادی در گذشته از نیترات نقره استفاده می شد ولی امروزه برای پیشگیری پماد تتراسیکلین و اریترومایسین به کار می رود .
درمان :
Causes and Treatment for Pink Eye
در نوع گونوکوک ایزوله کردن نوزاد ، درمان وریدی آنتی بیوتیک ، کشت خون وکشت مایع نخاع وکشت از مادر و دادن سفتریاکسون یا سفوتاکسیم و چکاندن قطره های استریل ایزوتونیک نمکی و معاینه دقیق توسط چشم پزشک توصیه می شود.
درنوع پسودومونا ایزوله کردن نوزاد و انجام کشت و درمان داخل رگی سفتازیدیم و جنتامایسین و معاینه دقیق توسط چشم پزشک توصیه می شود.
در نوع استافیلوکوک ایزوله کردن نوزاد وانجام کشت های مختلف و درمان سیستمیک متی سیلین
در نوع کلامیدیا درمان موضعی موثر نیست درمان خوراکی اریترومایسین در 4 دوز به مدت 14 روز چون 20 % عود می کند یک دوره دوم آنتی بیوتیک ممکن است لازم شود .
در سایر باکتری ها چکاندن قطره های موضعی وآنتی بیوتیک های موضعی مثل باسیتراسین ، نئو مایسین ، پلی میکسین ، هر 6 ساعت به مدت 7-10 روز
Conjunctivitis is the term used to describe inflammation of the conjunctiva—the thin, filmy membrane that covers the inside of your eyelids and the white part of your eye (sclera).
Conjunctivitis is most commonly referred to as red or “pink” eye.
The conjunctiva, which contains tiny blood vessels, produces mucus to coat and lubricate the surface of your eye.When the conjunctiva becomes irritated or inflamed, the blood vessels become larger and more prominent, making your eye appear red. Conjunctivitis may occur in one or both eyes.
Bacterial (bak·tee·ree·uhl) conjunctivitis
Symptoms of conjunctivitis include:
inflammation of the eye
increased tearing
soreness of the eye
foreign body sensation
itchiness of the eye
hazy or blurred vision due to mucous or pus
excess mucous (pus)
crusting of eyelashes in the morning.[1]
What causes conjunctivitis?
- Infection is the most common cause. - Allergy is another common cause. For example, many people with hay fever (allergic to pollen) have red and inflamed conjunctiva. - Irritant conjunctivitis sometimes occurs. For example, your conjunctiva may become inflamed after getting some shampoo in your eyes. The chlorine in swimming baths is a common cause of mild irritant conjunctivitis. The rest of this leaflet is about conjunctivitis caused by infection.[2]
What are the most common causes of conjunctivitis in childhood?
Conjunctivitis is an inflammation of the conjunctiva which is usually caused by infection or allergy. It is frequently referred to as pink eye and is the most common acute eye disorder seen by primary care pediatricians and family physicians.
What are the characteristics of allergic conjunctivitis?
Allergic conjunctivitis is characterized by ocular redness and itching. Tearing (clear tears), crusting of the eye lids and photophobia may also be seen. The condition is often recurrent, and seasonal. Children who have allergic conjunctivitis often have a history of other atopic diseases, particularly allergic rhinitis, eczema or asthma.
What are the characteristics of an infectious conjunctivitis?
Infectious conjunctivitis may be bacterial or viral. Bacterial conjunctivitis is twice as common as viral conjunctivitis. Typically in bacterial conjunctivitis the eye is red, there is a purulent discharge, the affected child is often a pre-schooler and there may be an associated otitis media. In viral conjunctivitis there is redness, clear tearing or crusting, usually occurs in an older school age child, and is often associated with pharyngitis.
What organisms are commonly involved in bacterial conjunctivitis?
The most common bacterial organisms causing conjunctivitis are Haemophilus Influenzae and Streptococcus pneumoniae. H. Influenzae conjunctivitis occurs in 40 to 50% of cases and is more likely to be associated with an accompanying otitis media than other organisms. S. Pneumoniae accounts for about 10% of cases and other organisms (Staphylococcus aureus, Bacteroides and Moraxella catarrhalis) account for the remainder.
What is the most common cause of viral conjunctivitis?
Adenovirus conjunctivitis is the most common cause of viral conjunctivitis and may account for up to 20% of infectious conjunctivitis. Outbreaks of adenoviral conjunctivitis have been linked to contaminated equipment in ophthalmology clinics and to swimming pools.
Why is there a need to distinguish viral from bacterial conjunctivitis?
Viral and other non-purulent types of conjunctivitis do not require antimicrobial treatment. Often these children are treated mistakenly for prolonged periods of time with both topical and systemic antibiotics with persistence of the red eye. In some situations the topical antibiotic itself may cause an allergic reaction resulting in a persistent red eye.
What is the pathogenesis of infectious conjunctivitis?
In children the joint communication of the conjunctival sac with the middle ear and nasopharynx probably accounts for the frequent association of otitis media and pharyngitis with acute conjunctivitis.
What is the differential diagnosis of acute conjunctivitis?
In the child with a non-purulent conjunctivitis, one should think of Kawasaki disease, Lyme disease, juvenile rheumatoid arthritis orSteven's Johnson syndrome. When there is decreased vision and light sensitivity the physician must think of uveitis. Trauma and allergic conjunctivitis account for the remainder of the differential diagnosis.
What is the treatment of choice for acute bacterial conjunctivitis?
Acute bacterial conjunctivitis is a self limited condition. However, the use of antibiotic treatment is recommended because it hastens healing considerably and it eradicates the bacterial pathogen allowing children to return to daycare centers and schools within 24 hours of treatment. Topical treatment with polymyxin-bacitracin, garamycin or other suitable topical antimicrobials should be used. There is usually no need to use topical treatment for more than 2 to 5 days when complete resolution should have occurred. Treatment should be applied to both eyes, even if only one eye appears to be infected. Topical application should be applied four times a day.
What approach should be used if the purulent discharge persists despite topical treatment?
If there is persistent eye discharge after Day 4 or 5 of treatment then one needs to consider an alternative diagnosis. The most common occurrence is that of an associated otitis media which has not been recognized or has subsequently developed and requires the use of an oral systemic antibiotic. This occurs most frequently in H. influenzae conjunctivitis. An oral antibiotic which has activity against beta lactamase producing organisms should be used.
Conjunctivitis In Children - Kids Health NZ
What is the treatment for viral conjunctivitis?
Non-purulent viral conjunctivitis requires no treatment.
What is the treatment for allergic conjunctivitis?
Allergic conjunctivitis can be treated with an ophthalmic preparation containing a topical decongestant with or without antihistamine. Prevention of allergic conjunctivitis in susceptible individuals is best treated with topical sodium chromoglycate.[3]
Infectious conjunctivitis is highly contagious, soteach kids to wash their hands well and often with warm water and soap. They also should not share eye drops, tissues, eye makeup, washcloths, towels, or pillowcases.
Be sure to wash your own hands well after touching an infected child’s eyes, and throw away items like gauze or cotton balls after they’ve been used. Wash towels and other linens that the child has used in hot water separately from the rest of the family’s laundry to avoid contamination.
If you know your child is prone to allergic conjunctivitis, keep windows and doors closed on days when the pollen is heavy, and dust and vacuum often to limit allergy triggers. Irritant conjunctivitis can only be prevented by avoiding the irritating causes.
Screening and treating pregnant women for STDs can prevent many cases of pinkeye in newborns. A pregnant woman may have bacteria in her birth canal even if she shows no symptoms, which is why prenatal screening is important.
Conjunctivitis is a common eye condition that affects children, especially under 5 years of age. It can either be caused by an infection or by an allergy. Infectious conjunctivitis is contagious and may spread to other household members. Allergic conjunctivitis is more common in children with allergies such as hay fever.
Neonatal conjunctivitis and dacryocystitis
If your child has conjunctivitis, they may have:
a red or pink eye (or both eyes)
redness behind the eyelid
swelling of the eyelids, making them appear puffy
excessive tears
a yellow-green discharge from the eye which dries when your child sleeps, causing crusting around the eyelids
a gritty feeling (like there is sand in the eye)
itchiness of the eyes and eye rubbing
children with allergic conjunctivitis almost always rub their eyes excessively. They may also have an itchy or runny nose and sneezing
Your child does not need to be excluded from school or childcare if they have conjunctivitis.[8]
You need to contact a doctor or nurse today.
If your child has any of the following:
+ Severe pain in eyes
+ Extreme sensitivity to light (photophobia)
+ Changes in vision including flashing lights (vision can appear blurred or misted because of discharge smeared over the surface of the eye, but this will usually clear on blinking or wiping the eyes)
+ If you notice any redness, swelling or puffiness around the eye or eyelids.
+ Severe headache
+ Persistent vomiting
+ Blisters develop on the skin next to the eye
+ Babies under 28 days with a red eye(s) or lots of pus from their eye(s) - note although a sticky eye due to a blocked tear duct is a very common condition in babies (and does not require medical review), this condition does not cause a red eye
+ Is finding it hard to breathe
+ Seems dehydrated (sunken eyes, drowsy or not passed urine for 12 hours)
+ Is becoming drowsy (excessively sleepy) or irritable (unable to settle them with toys, TV, food or picking up) - especially if they remain drowsy or irritable despite their fever coming down
+ Has extreme shivering or complains of muscle pain
+ Is 1-3 months of age with a temperature of 38°C / 100.4°F or above, or 3-6 months of age with a temperature of 39°C / 102.2°F or above (but fever is common in babies up to 2 days after they receive vaccinations)
+ Continues to have a fever of 38.0°C or above for more than 5 days
+ Is getting worse or if you are worried bacterial conjunctivitis does not improve after 24 hours of antibiotic use
You need urgent help.If your child has any of the following:
- Becomes pale, mottled and feels abnormally cold to touch
- Is going blue around the lips
- Too breathless to talk / eat or drink
- Has a fit/seizure
- Becomes extremely agitated (crying inconsolably despite distraction), confused or very lethargic (difficult to wake)
- Develops a rash that does not disappear with pressure (see the 'Glass Test')
- Is under 1 month of age with a temperature of 38°C / 100.4°F or above
Conjunctivitis is an inflammation of the conjunctiva, which is the mucous membrane covering the white of the eyes and the inner side of the eyelids.
Inflammation is seen as reddish change in the periphery of the eye often accompanied by a pus-like discharge.
Signs and symptoms of conjunctivitis[5]
If your child has conjunctivitis, they may have:
a red or pink eye (or both eyes).
redness behind the eyelid.
swelling of the eyelids, making them appear puffy.
excessive tears.
a yellow-green discharge from the eye which dries when your child sleeps, causing crusting around the eyelids.
a dislike of bright lights (photophobia).
a gritty feeling (like there is sand in the eye).
itchiness of the eyes and eye rubbing.
It usually affects both eyes at the same time – although it may start in one eye and spread to the other after a day or two. It may be asymmetrical, affecting one eye more than the other.
There are many causes and the treatment will depend upon the cause.
Conjunctivitis is a common eye condition. It's not serious, but it can be uncomfortable and irritating.[1]
How is conjunctivitis diagnosed
Classification
Classification can be either by cause or by extent of the inflamed area.
By cause
Allergic conjunctivitis
Bacterial conjunctivitis
Viral conjunctivitis
Chemical conjunctivitis
Neonatal conjunctivitis is often defined separately due to different organisms
By extent of involvement Blepharoconjunctivitis is the dual combination of conjunctivitis with blepharitis (inflammation of the eyelids).
Keratoconjunctivitis is the combination of conjunctivitis and keratitis (corneal inflammation).
Episcleritis is an inflammatory condition that produces a similar appearance to conjunctivitis, but without discharge or tearing.[2]
Treatments for various types of conjunctivitis
Bacterial conjunctivitis can be treated by antibiotics
?Does My Kid Have Pink Eye
Bacterial conjunctivitis in adults is always caused by infections such as staphylococcus and streptococcus. In children, a common cause is Haemophilus influenza bacteria. Besides eye cleanser and artificial tears for relieving symptoms, the doctor will also prescribe standard antibiotics to treat bacterial conjunctivitis. In most cases, antibiotics are enough and a sample evaluation is unnecessary.
Hereditary gonococcal conjunctivitis requires injection of antibiotics
Newborn babies are at high risk of gonococcal conjunctivitis, which is caused via the contact with their mothers. This type of conjunctivitis results from sexually transmitted diseases on pregnant women, who should be treated with antibiotics to prevent the infection from being passed to their children. Caused by either birth-related bacteria or pink eye exposure, some cases of gonococcal conjunctivitis even occur after several weeks of birth.
Once a child is diagnosed with gonococcal conjunctivitis, the most common treatment is to take an intravenous injection of antibiotics through either veins or muscles. Another treatment is applying silver nitrate and antibiotic ointments to its eye within an hour after birth.
Viral conjunctivitis can be relieved by antihistamine and steroids
Viral conjunctivitis has symptoms such as watery mucus discharge and eye redness. This type of conjunctivitis usually spreads through respiratory infection, so that children with a cold are more likely to be affected. As a result, pink eye epidemics may be aroused among school children via sneezing and coughing. Other reasons that may cause viral conjunctivitis include virus-based illness such as measles and mumps. Viral conjunctivitis can not be cured, only treatments for symptom relief are available. Antihistamine is used to relieve eye itchiness and irritation, and vasoconstrictors are effective for reducing redness. Steroids are also used to control symptoms and speed up recovery, while they may cause cataracts or glaucoma. Most cases of viral conjunctivitis will go away on its own within several days or weeks.
Allergic conjunctivitis require eye drops and mast-cell stabilizer
Allergic conjunctivitis also has various symptoms, including itchiness, stringy mucous discharge and red eye, stuffy and runny nose. People with allergic conjunctivitis can usually get relief from ordinary eye drops, which are helpless for individuals with severe conditions. Serious conjunctivitis should be treated with steroid eye drop medications at the beginning and mast-cell stabilizer for regular use. Due to potential side effects such as cataracts, the use of steroid must be under careful monitoring.
Giant papillary conjunctivitis calls for the use of GP contact lenses
Giant papillary conjunctivitis (GPC) is always found in people wearing soft contact lenses. Other potential risks of GPC include artificial eye and an exposed suture. People with GPC always tear much, produce significant mucus and get itching eyes or eyelid bump. For symptom relief, saline solution can be used to wash the eye’s surface. There are still some remedies for GPC involving soft contact lenses. The most effective way is to remove contact lenses, along with their abnormal immune response. For those persisting in lenses wearing, mast-cell stabilizers may be used. To avoid the recurrence of GPC, it is encouraged to can wear RGP lenses and use strict lenses hygiene.[3] eResearch by Navid Ajamin -- spring 2012
What are the risk factors for conjunctivitis?
There are many possible risk factors for conjunctivitis, including: [4]
Hand hygiene. Conjunctivitis can easily spread from your hands to your face. If you aren’t washing or sanitizing your hands frequently, you might be more likely to develop this condition.
Age. Viral conjunctivitis is common in adults and children, while bacterial conjunctivitis is far more likely in children under age 4. There’s also a higher risk for people in their 20s, but experts aren’t certain why.
Time of year. Allergic conjunctivitis is much more common in spring and summer. Infectious forms of conjunctivitis are also more common during cold and flu season.
Medical history. Having seasonal allergies or allergy-related conditions like eczema or atopic dermatitis can make you more likely to develop conjunctivitis.
Sharing personal items. The contagious forms of conjunctivitis spread easily on certain objects, especially eye-related items like cosmetics and contact lens containers. The contagious forms can also spread easily on cloth, like washcloths, towels and pillowcases.
With summer fast approaching, parents should be keeping a closer eye on their children's vision. According to research from the 2010 Transitions Healthy Sight Survey, which was released to coincide with World Sight Day on 14 October 2010, only a third (34%) of South African parents actively protect their children's eyes from harmful ultraviolet (UV) rays. Worrying considering children spend - on average - three times more time outdoors than adults and yet only one in 10 children wearUV protective sunglasses.
"Most parents know the irreversible damage UV rays can have on the skin but few are aware of the potential danger repeated UV exposure poses to eye health," says Dr Caradee Wright, senior researcher at the Council for Scientific and Industrial Research in Pretoria. Whilst eyes of all ages need UV protection, children’s crystalline lenses are incapable of filtering out UV light. As the damaging effects of UV rays are cumulative, extended exposure over many years can lead to the early onset of cataracts and macular degeneration later in life.
UV damage is cumulative eResearch by Navid Ajamin -- spring 2012
Increased life expectancy of today’s young people further adds to a child’s eventual risk of developing vision problems. Therefore, protecting the eyes at an early age is essential. Proper lenses can safely block UV radiation and wearing a hat can cut by half the amount of UV rays that reach the eyes.
"Parents need to be informed that UV damage is cumulative and more often than not only detected much later in adulthood. Early prevention of extended UV exposure is better than the possibility of a cure in the long term," adds Wright. "Parents should also bear in mind that UV protection is needed year-round, even on cloudy days as over 90% of UV rays can penetrate light clouds."
In addition, the Transitions Healthy Sight Survey revealed that only 10% of South African children wear spectacle lenses with built-in UV protection. "This is not entirely surprising since most adults are not aware of the benefits of premium lens options for themselves, much less for their children," says Riette Botha, business manager for Transitions Optical South Africa (SA).
"Young eyes are sensitive to bright sunlight and glare. As Transitions® adaptive lenses automatically adapt to changing light it’s easier for children to see better while significantly reducing the discomfort of squinting, eye strain and eye fatigue."
Eyewear for children has advanced significantly in recent years and can now address unique visual needs as well as long-term eye health concerns like never before.
Eyewear should provide 100% protection
All types of eyewear, including sunglasses and prescription spectacles, should provide 100% UV protection.
"If your child does need everyday corrective spectacles, Transitions® adaptive lenses, which automatically adapt from clear indoors to dark outdoors when exposed to UV light, are the ideal option. Transitions® adaptive lenses automatically provide 100 percent protection against harmful UVA and UVB rays. "Transitions® adaptive lenses can also help boost a child's willingness to wear glasses," adds Botha.
Vision plays a key role in a child’s early functional, educational and social development and approximately 80% of learning in a child’s first 12 years comes from the eyes3. Changes in children’s vision can occur without parents noticing them.
This is why it is recommended children undergo regular eye exams as they grow and as their eyes continue to change and adapt.
Furthermore, conditions such as myopia, hypermetropia and astigmatism, all of which can have an impact on a child's ability to learn and perform in the classroom, are easily detected by means of an eye exam.
Educating children today about their vision and how to better take care of their eyes can help prevent irreversible eye damage in future.
Did you know?
One child goes blind every minute in the world. (World Health Organisation)
More than 12 million children aged five to 15 are visually impaired because of uncorrected refractive errors (near-sightedness, far-sightedness or astigmatism). (World Health Organisation)
The clear crystalline lens of the child under age 10 transmits more than 75% of incident UV rays, compared to only 10% at age 30. (Healthy Sight Counseling and Children, 2007)
Sunglasses that have not been treated for UV rays may be more detrimental to your eyes than not wearing sunglasses at all. Dark lenses reduce the amount of light entering the eye, causing the pupil to dilate. This exposes the inside of your eye to more UV radiation than without the sunglasses.
Many surfaces reflect the sun’s rays and add to the overall UV exposure, e.g. grass, soil and water reflect less than 10% of UV radiation; fresh snow reflects up to 80%; dry beach sand reflects 15%, and sea foam reflects 25%.
UV increases by 4% for each 300 metre increase in altitude.
Children spend much time in school, and UV radiation exposure during the school years contributes significantly to total lifetime sun exposure.
بیشتر ناهنجاری های بینایی، بین سنین 4 تا 9 سالگی قابل تشخیص هستند...
البته به شرطی که گوش به زنگ و دقیق باشید!
آیا فرزندتان خوب میبیند؟
نشانه هایی برای والدین :با گذشت ماه ها، بینایی نوزاد ظرافت بیشتری پیدا میکند، زیرا بیشتر مورد استفاده قرار میگیرد. هر نشانۀ غیر طبیعی، که در رفتار نوزاد دیده شود، باید شما را به سمت مراجعه به بینایی سنج هدایت کند.
شما میتوانید بینایی نوزادتان را با دو تست متفاوت بسنجید: در یکی از این تست ها، یک جسم نورانی را به سمت صورت نوزاد ببرید (اگر چشمانش را باز و بسته کرد، یعنی میبیند) و ببینید که آیا او میتواند یک شی را که رنگ ها متضاد (سیاه و سفید) دارد دنبال کند یا نه. این دو تست ساده میتوانند نشان دهندۀ یک نقص در بینایی باشند یا به تشخیص یک بیماری مانند آب مروارید مادرزاد رهنمون شوند. سپس، از 4 ماه به بعد دیگر زمان آن رسیده که نوزادتان را پیش یک بینایی سنج ببرید.
نشانه های ناهنجاری بینایی:چه زمانی باید به پزشک مراجعه کرد؟
اگر کسی در خانواده تان وجود دارد که دچار مشکل بینایی است.
اگر نوزاد بزرگتر از سه ماه تان هنگامی که چهرۀ افراد آشنا را میبیند، نمیخندد.
اگر نوزاد چند هفته ای تان نگاهش را به سمت نور برنمیگرداند یا به نظر میرسد از نگاه کردن به منبع نور خودداری میکند.
اگر اشیا را نمیگیرد یا آنها را در دهانش نمیگذارد.
اگر نگاه ها را دنبال نمیکند.
اگر زمانی که شروع به خوب راه رفتن کرد، مدام به اشیا و مبل ها برخورد کند.
اگر از 6 ماهگی به بعد به میزان زیادی چشمش چپ باشد.
چه طور میتوان مشکلات مختلف بینایی نوزاد را تشخیص داد؟ ضعف بینایی: تسلط بینایی یک چشم که شدت بینایی چشم دیگر را کاهش میدهد. هر چند وقت یک بار یک چشم نوزاد را ببندید و بعد از مدتی چمش دیگر را و نتیجۀ آن را مشاهده کنید. اگر احساس میکنید که با این کار نوزاد خیلی اذیت میشود، با یک متخصص در این باره صحبت کنید. دوربینی چشم: عملاً همۀ نوزادها با چشم های دوربین متولد میشوند. این یک تأخیر در تکمیل بینایی است که دید نامناسب از نزدیک را با خود به همراه دارد اما نوزاد دور را خوب میبیند، با بزرگ شدن نوزاد این مشکل حل میشود. با این حال دقت داشته باشید که نوزادتان چه زمانی به اشیا نگاه میکند و به آنها دست میزند. eResearch by Navid Ajamin -- spring 2012 نزدیک بینی: در این حالت نوزاد نزدیک را خوب و دور را بد میبیند. اگر او برای دیدن چیزهایی که از او فاصله دارند، چشم هایش را چندین بار باز و بسته میکند و تمایل دارد که اسباب بازی هایش را به چشمش خیلی نزدیک کند، حتماً با یک متخصص مشورت کنید. آستیگماتیسم: این مشکل در نتیجۀ شکل گیری نامناسب قرنیه به وجود میآید. یکی از نشانه های گویای آن، ورم ملتحمۀ پرتکرار است. لوچی: این مشکل که خود را با انحراف ارثی محور یک چشم نسبت به چشم دیگر نشان میدهد، ممکن است همگرا یا واگرا باشد. اگر شما مورد لوچی در خانواده تان دارید، با یک متخصص بینایی مشورت کنید. اگر چه این مشکل تا سه ماهگی نوزاد به علت اینکه مغز هنوز نمیتواند تصاویر چشم ها را روی هم منطبق کند، تقریباً عادی است، اما در صورت تداوم این عارضه از این سن به بعد باید با پزشک مشورت کنید. زیرا علاوه بر مشکل ظاهری، چشم لوچ بد میبیند. اگر بعد ها این مشکل حل نشود، خطر شدید شدن مشکل و طول کشیدن بیشتر دورۀ درمانی وجود دارد.
تکامل بینایی نوزاد طی چند ماه بعد از تولد: نوزاد میبیند اما نه به طور کامل. او نمیتواند تطابق دهد و رنگ ها را از هم تشخیص نمیدهد، اما این شرایط برای تشخیص چهرۀ شما کفایت میکند. او میتواند نگاهش را تثبیت کند یا با نگاهش، چیزی را که مقابلش حرکت میدهید، دنبال کند. طی هفته های اول، او ممکن است حرکات نامنظم چشم داشته باشد زیرا ماهیچه های چشمی نیروی کامل شان را تا قبل از 6 ماه به دست نمیآورند در 3 ماهگی: به نظر میرسد که چشم نوزاد چپ شده است، او گه گاه با یک چشم و گه گاه با چشم دیگر نگاه میکند در 4 ماهگی: او بیشتر و بیشتر تطابق پیدا میکند، چشم راست و چشم چپش دیگر جدا از هم کار نمیکنند، دید به وسیلۀ هر دو چشم از این زمان، آغاز میشود. در 1 سالگی: شدت بینایی کودک در این سن 4/10e است. در 18 ماهگی: او میتواند چیزهای کوچک را مشاهده کند، اما برای اینکه ظرفیت بینایی او مانند افراد بزرگسال بشود، باید تا 4 الی 5 سالگی صبر کرد.(۱)
مشکلات بینایی در نوزادان نارس : premature baby
تکامل بینایی در نوزادان نارس کمی بیشتر از نوزادانی که به موقع بدنیا آمده باشند طول می کشد. احتمال ایجاد استرابیسم و آمبلیوپی در نوزادانی که قبل از هفته ۳۵ حاملگی بدنیا آمده باشند ۳۰% بیشتر است. هر چه نوزاد زودتر از زمان طبیعی بدنیا بیاید این احتمال افزایش می یابد. نوزاد باید کاملا به نور روشن (مثلا لامپ) و یا آویز هایی که معمولا بالای سر نوزادان آویزان می کنند توجه کند. اگر در ۳ ماهگی جسم را جلو چشم نوزاد بگیرید و آن را از یک سمت آهسته به سمت دیگر ببرید و نوزاد قادر به دنبال کردن آن با چشم نباشد بهتر است مورد معاینه قرار گیرد. البته در بعضی موارد تکامل بینایی دیرتر رخ می دهد که به آن تأخیر در تکامل بینایی می گویند.(۲)
Does prematurity affect vision?
One in ten very premature infants — those born at less than 30 weeks gestation — are affected by retinopathy of prematurity (ROP), the leading cause of childhood blindness.(5)
YOUR PREMATURE BABY
Babies born preterm (before 37 weeks) are still developing their sense of vision. Babies born before the age of 32 weeks are unable to limit the amount of light entering their eyes even when their eyes are closed. It is therefore important to protect premature babies from bright lights.
EFFECTS OF VISION ON YOUR BABY
Babies born at term have a preference for looking at faces. Older premature babies too can fixate on your face briefly if you are holding them closely (approximately 25-30cm or 10-12 inches from your face), as they are very near sighted at this stage. Your baby is likely to have an incubator cover over their incubator whilst in intensive care. This reduces their exposure to bright light and aims to recreate the conditions of the womb. As your baby matures these incubator covers are pulled back. It is important that you enjoy your baby. Talk to them, smile, be expressive; your baby learns from watching your facial expressions.(3)
When can a premature baby see clearly?
Babies are born with their eyes almost fully developed, but they do not see clearly until their second year. This can take a little longer for premature babies. Babies can see from birth; however, initially their vision is very limited because the retina is not completely developed.(4)
Common vision problems in children
If your child has a vision problem, it could affect their school performance. Eye exams and treatment can improve:
Learning.
Testing.
Class participation.
Behavior.
Self-confidence.
Parents and teachers can help children by being aware of common vision problems.
Refractive errors
Refractive errors occur when light doesn't correctly focus on the retina (the light-sensitive tissue at the back of the eye). This condition causes blurred vision. This eye condition includes:
Myopia (nearsightedness)
Hyperopia (farsightedness)
Astigmatism (when the cornea or lens has a different shape than normal)
If you notice your child squinting, rubbing their eyes, or complaining of headaches after doing schoolwork, have their vision checked
Amblyopia (lazy eye)
This condition occurs when vision in one eye is reduced because of a communication error in the brain. The brain will rely more and more on the stronger eye, while vision in the weaker eye gets worse.
Strabismus (crossed eyes)
This eye condition can affect one or both eyes. When a child has strabismus, their eyes do not focus on the same object at the same time. As a result, their eyes have trouble maintaining the correct position.
Convergence insufficiency
This eye condition affects how the eyes work together when looking at objects close up. Convergence insufficiency can cause blurry or double vision while looking at any object close up, like a book or digital device.
If you notice your child squinting, rubbing their eyes, or complaining of headaches after doing schoolwork, have their vision checked. An eye doctor can check for eye conditions and other vision problems and provide treatment if needed.(6)
دو تصور غلط در مورد معاينه چشم وجود دارد. يكي اين است كه اگر خوب مي بينيد نيازي به معاينه چشم نداريد و ديگري اينكه "تست بينايي" كه حدت بينايي را با استفاده از تابلو هاي مخصوص اندازه گيري مي كند (مشابه تست هاي بينايي كه در هنگام اخذ گواهينامه رانندگيانجام مي شود) همان معاينه چشمي است با اسمي ديگر. اما بايد توجه داشت كه چشم پزشك در واقع علاوه بر تست بينايي، چشم شما را از نظر بيماري هاي ديگري نيز كه ممكن استعلائم زودرسنداشته باشند ولي نياز به درمان زودرس دارند معاينه مي كند. بنابراينمعاينه كامل چشمي بسيار بيشتر از يك تست بينايي است.
چه كساني بايد مورد معاينه چشمي قرار گيرند؟
صرف نظر از سن و سلامت جسماني، هر شخصي بايد بصورت دوره اي و منظم مورد معاينه چشمي قرار گيرد. در بزرگسالان معاينه چشمي از جهت درست بودن شماره عينك و تشخيص زوردس بيماري ها اهميت دارد.در كودكان، معاينه چشمي نقش بسيار مهمي در تكامل بينايي كودك دارد.
از آنجاييكه بينايي نقش مهمي در فرايند يادگيري كودكان دارد، اهميت معاينات دوره اي در كودكان دو چندان است. مشكل بينايي كودك گاهي خود را بصورت افت تحصيلي و مشكل در انجام تكاليف مدرسه نشان مي دهد. در بسياري موارد، كودكان به اين دليل كه نمي دانند ديد "طبيعي" چگونه بايد باشد شكايتي از ديد خود ندارند. اگر كودك شما از نظر درسي در مدرسه مشكل دارد و يا در خواندن و يادگيري دچار مشكل است حتماً بايد جهت اطمينان از عدم مشكلات چشمي معاينه شود.
در معاينه چشم چه مشكلاتي مورد توجه قرار مي گيرند؟
مشكلاتي كه چشم پزشك در معاينه چشمي بدانها توجه مي كند
عبارتند از:
عيوب انكساري: شامل دوربيني، نزديك بيني، آستيگماتيسم، ...
تنبلي چشم (آمبليوپي): اين مشكل در موارد استرابيسم و يا اختلاف زياد بينايي دو چشم رخ مي دهد. در اين وضعيت مغز تصوير گرفته شده از چشم مشكل دار را ارسال نمي كند. آمبليوپي در صورت عدم درمان ممكن است باعث اختلال در تكامل بينايي شده و اختلال دائمي بينايي را بهمراه داشته باشد. اين اختلال معمولاً با بستن چشم بدون مشكل براي مدتي مشخص درمان مي شود.
استرابيسم (انحراف چشم): چشم پزشك چشم بيمار را از نظر هماهنگي حركتي و وضعيت قرار گيري نسبت به يكديگر بررسي مي كند. استرابيسم مي تواند سبب اختلال در درك عمق و آمبليوپي شود.
بيماريهاي چشمي: بسياري از بيماريهاي چشمي نظير گلوكوم و مشكلات ناشي از ديابت در مراحل اوليه علائم واضحي ندارند. چشم پزشك در معاينه چشمي به اين بيماري ها توجه كرده و در صورت برخورد با اين علائم درمان هاي اوليه را آغاز مي كند. در بسياري موارد تشخيص و درمان زودرس بيماريها سبب كاهش عوارض و از دست دادن دائمي ديد مي شود.
بيماريهاي ديگر: معاينه عروق ته چشم، پرده شبكيه و ديگر قسمت هاي چشم مي تواند ابتلا بيمار به بيماري هاي غير چشمي نظير فشار خون، ديابت، چربي بالا و بعضي بيماري هاي ديگر را نشان دهد.
معاينه چشمي به چه فواصلي بايد انجام شود؟ How Often Should You Get an Eye Exam
چشم پزشكان توصيه مي كنند كه هر فردي بسته به داشتن ريسك فاكتور و سلامت جسماني هر 1 تا 3 سال يكبار معاينه كامل چشمي شود.
كودكان: اين زمان در كودكان متفاوت است. تخمين زده مي شود كه از هر 20 كودك پيش دبستاني و هر 4 كودك دبستاني 1 كودك مشكل چشمي دارد كه در صورت عدم درمان مي تواند سبب كاهش دائمي بينايي شود. كودكاني كه علائمي نداشته و ريسك پاييني دارند بايد در 6 ماهگي، 3 سالگي و قبل از ورود به مدرسه معاينه كامل چشمي شوند. اين كودكان پس از آن بايد هر 2 سال مورد معاينه قرار گيرند.
اما كودكان داراي ريسك فاكتور مشكلات بينايي، نياز به معاينات بيشتري دارند.
بعضي از اين ريسك فاكتورها عبارتند از:
سابقه خانوادگي بيماري هاي چشمي family history of ocular diseases
سابقه صدمات چشمي the history of eye injuries
تأخير در تكامل developmental delay in children
انحراف چشم unusual ocular deviation
تولد زودرسpremature birth
كودكاني كه از عينك يا كنتاكت لنز استفاده مي كنند اغلب نياز به معاينات سالانه دارند تا در صورت تغيير در شماره چشم، عينك آنها اصلاح شود.
بزرگسالان: بطور كلي، بسته به ميزان تغييرات بينايي و سلامت جسماني، بزرگسالان بايد تا سن 40 سالگيهر 2 تا 3 سال تحت معاينه كامل چشمي قرار گيرند. در بيمارني كه به بيماري هايي نظير ديابت و فشار خون مبتلا هستند معاينات بيشتري توصيه مي شود زيرا اين بيماري ها تاثير سويي بر بينايي دارند.در افراد بالاي 40 سال بهتر است معاينه چشميهر 1 تا 2 سال صورت گيرد. زيرا بعضي بيماري هاي نظير پير چشمي، كاتاراكت و دژنراسيون ماكولا با افزايش سن اتفاق مي افتند.از آنجا كه ريسك بيماري هاي چشم با افزايش سن بالا مي رود افراد بالاي 60 سال بازهر سال معاينه شوند.
Optometrists(OD)and ophthalmologists(eye MD)use a wide variety of tests and procedures to examine your eyes. These tests range from simple ones, like having you read an eye chart, to complex tests, such as using a high-powered lens to visualize the tiny structures inside of your eyes.
What is the normal eyesight of a child
An eye examinationis a series of tests performed by an ophthalmologist (medical doctor), optometrist, or orthoptist, optician (UK), assessing vision and ability to focus on and discern objects, as well as other tests and examinations pertaining to the eyes.
eye and vision tests that you are likely to encounter during a comprehensive eye exam:
Ocular Motility (Eye Movements) Testing ; Stereopsis (Depth Perception) Test
Autorefractors And Aberrometers ; Peripheral Visual Field Test
Applanation Tonometry ; Contrast sensitivity Test
Non-Contact Tonometry ; Fluorescein Angiogram
Contact Lens Fittings ;Color Blindness Test
Retinal Tomography ;The Glaucoma Test
Visual Acuity Tests ; Keratometry Test
Visual Field Test ; Slit Lamp Exam
Pupil Dilation ; Retinoscopy
Ultrasound ;Cover Test
Refraction
Visual Ability
The basic mechanical skills of the visual system are: eye movements, which are important for following a moving object or looking from one object to another, as well as the ability to look at a single object, whether still or moving, for as long as is necessary; eye teaming, which refers to both eyes pointing at the same thing at the same time; without this ability there can be confusion and disorientation in processing visual information for meaning and response; and focusing, which is the ability to see clearly at any distance for any period of time with minimal effort. Other very important aspects of visual function are peripheral visual awareness and eye/hand coordination.
Eye health evaluation
A wide variety of microscopes, lense, and digital technology will be used to assess the health of all the structures of the eye and the surrounding tissues. Dilating eye drops are often used to temporarily widen the pupil for better views of the structures inside the eye. In addition to measuring the pressure inside of the eye, this also is part of the eye exam where a doctor of optometry can detect otherwise unknown eye and systemic diseases.
Supplemental testing
Additional testing may be needed based on the results of the previous tests to confirm or rule out possible problems, to clarify uncertain findings, or to provide a more in-depth assessment.
At the completion of the examination, the doctor will assess and evaluate the results of the testing to determine a diagnosis and develop a treatment plan. He or she will discuss with you the nature of any visual or eye health problems found and explain available treatment options. In some cases, referral for consultation with, or treatment by, another doctor of optometry or other health care provider may be indicated. If you have questions about any diagnosed eye or vision conditions, or treatment recommendations, don't hesitate to ask your doctor for additional information or explanation. eResearch by Navid Ajamin -- spring 2012
The 8-Point Eye Exam
The key to any examination is to be systematic and always perform each element.
1.Visual acuity In the clinic, visual acuity is typically measured at distance. Otherwise, in a consult setting outside of the clinic, it’s measured at near. Don’t forget to have a near card with you. Make sure the patient is wearing his or her correction. Always have a pair of +3.00 readers with you, as many people in the emergency room won’t have their glasses with them. A pinhole occluder will also reduce the impact of uncorrected refractive error. If the patient is unable to see the biggest optotype on the card, the progression (from better to worse) is counting fingers (CF), hand motions (HM), light perception (LP) with projection, LP without projection and no light perception (NLP). For children who are too young to use Allen pictures, employ the “central, steady, maintain (CSM)” approach. Central: Is the corneal light reflex in the center of the pupil? Steady: Can the patient continue fixating when the light is slowly moved around? Maintain: Can the patient maintain fixation with the viewing eye when the previously covered eye is uncovered?
2.Pupils Look for anisocoria. If present, carefully check the pupil size in both well-lit and dark conditions. Check the reactivity of each pupil with a penlight or Finoff transilluminator. Use the swinging flashlight test to look for a relative afferent pupillary defect.
MYOPIA CONTROL: YOUR CHILD’S VISION
3.Extraocular motility and alignment Have the patient look in the six cardinal positions of gaze. Test with both eyes open to assess versions — repeat monocularly to test ductions. Use the cover/uncover test to assess for heterotropias. Use the alternate cover test to assess for the total amount of deviation. This amount minus any heterotropia is the amount of heterophoria.
4.Intraocular pressure Goldmann applanation tonometry is the gold standard and should be used in the clinic whenever possible. Outside of the clinic, Tono-Pen tonometry is much more practical. If you suspect a ruptured globe, skip this part of the exam.
5.Confrontation visual fields Assess each quadrant monocularly by having the patient count the number of fingers that you hold up. If acuity is particularly poor, have the patient note the presence of a light. Use the colored lid of an eyedrop bottle to define the position of a scotoma more accurately.
6.External examinationLook for any ptosis by measuring the margin-to-reflex distance, which is the distance from the corneal light reflex to the margin of the upper lid. Look for lagophthalmos. Note any unusual growths or lesions that may require a biopsy. Palpate lymph nodes and the temporal artery if indicated by the history or exam. Measure proptosis or enophthalmos with an exophthalmometer. Perform a full cranial nerve exam for patients with diplopia or other neurologic symptoms.
7.Slit-lamp examination Lids/lashes/lacrimal system: Normal anatomy and contours? Any lesions? Conjunctiva/sclera: White and quiet? Injection? Lesions? Cornea: Clear? Epithelial disruptions? Stromal opacities? Endothelial lesions? Anterior chamber: Deep? Cell or flare? Iris: Round pupil? Transillumination defects? Nodules? Lens: Clear? Nuclear, cortical or subcapsular cataract? Anterior vitreous: Inflammation? Hemorrhage? Pigmented cells?
8.Fundoscopic examinationOptic nerve: Cup-to-disc ratio? Focal thinning? Pallor? Symmetric? Macula: Foveal light reflex? Drusen, edema or exudates? Vessels: Contour and size? Intraretinal hemorrhage? Periphery: Tears or holes? Lesions? Pigmentary changes?
Understanding your vision and pinpointing the problems can be somewhat of a challenge at times.
What can sometimes be even more confusing is knowing what kind of eye exam to get: a comprehensive one or a regular one?
Knowing the difference between a comprehensive eye exam and a regular or routine eye exam is crucial in keeping your eyes healthy. It’s important to know which one to get done when it comes time to check your eyes.
The Difference Between a Comprehensive Eye Exam and a Regular One
A comprehensive eye exam normally takes about half an hour to an hour to complete, depending on how many exams you need to take. A comprehensive eye exam is a collection of a bunch of different tests used to diagnose disease and vision impairments.
Refraction
In physics, "refraction" is the mechanism that bends the path of light through the eye. In an eye exam, the term refraction is the determination of the ideal correction of refractive error. Refractive error is an optical abnormality in which the shape of the eye fails to bring light into sharp focus on the retina, resulting in blurred or distorted vision. Examples of refractive error are myopia, hyperopia, and astigmatism.
A refraction procedure consists of two parts: objective and subjective.
Objective refraction
An objective refraction is a refraction obtained without receiving any feedback from the patient, using a retinoscope or auto-refractor.
To perform a retinoscopy, the doctor projects a streak of light into a pupil. A series of lenses are flashed in front of the eye. By looking through the retinoscope, the doctor can study the light reflex of the pupil. Based on the movement and orientation of this retinal reflection, the refractive state of the eye is measured.
An auto-refractor is a computerized instrument that shines light into an eye. The light travels through the front of the eye, to the back and then forward through the front again. The information bounced back to the instrument gives an objective measurement of refractive error without asking the patients any questions.
Subjective refraction
A subjective refraction requires responses from the patient. Typically, the patient will sit behind a phoropter or wear a trial frame and look at an eye chart. The eye care professional will change lenses and other settings while asking the patient for feedback on which set of lenses give the best vision.
Cycloplegic refraction
Sometimes, eye care professionals prefer to obtain a cycloplegic refraction, especially when trying to obtain an accurate refraction in young children who may skew refraction measurements by adjusting their eyes with accommodation. Cycloplegic eye drops are applied to the eye to temporarily paralyze the ciliary muscle of the eye.
Retinal examination
Direct exam. Your eye doctor uses an ophthalmoscope to shine a beam of light through your pupil to see the back of the eye. Sometimes eyedrops aren't necessary to dilate your eyes before this exam.
Indirect exam. During this exam, you might lie down, recline in a chair or sit up.
What Else Can Your Eye Exam Include?
Your ophthalmologist may suggest other tests to further examine your eye. This can include specialized imaging techniques such as:
topography
fundus photos
fluorescein angiography (FA)
optical coherence tomography (OCT)
Each part of the comprehensive eye exam provides important information about the health of your eyes. Make sure that you get a complete examination as part of your commitment to your overall health.
These tests can be crucial. They help your ophthalmologist detect problems in the back of the eye, on the eye's surface or inside the eye to diagnose diseases early.
Eye testing for infants
Babies should be able to see as well as adults in terms of focusing ability, color vision and depth perception by 6 months of age.
To assess whether your baby's eyes are developing normally, the doctor typically will use the following tests:
Tests of pupil responses evaluate whether the eye's pupil opens and closes properly in the presence or absence of light.
"Fixate and follow" testing determines whether your baby's eyes are able to fixate on and follow an object such as a light as it moves. (Infants should be able to fixate on an object soon after birth and follow an object by the time they are 3 months old.)
Preferential looking involves using cards that are blank on one side with stripes on the other side to attract the gaze of an infant to the stripes. In this way, vision capabilities can be assessed without the use of a typical eye chart.
Recommended examination frequency for the pediatric patient
At-risk
Asymptomatic / low risk
Patient age (years)
At 6 to 12 months of age or as recommended
At 6 to 12 months of age
Birth through 2
At least once between 3 and 5 years of age or as recommended
At least once between 3 and 5
3 through 5
Before first grade and annually, or as recommended thereafter
Before first grade and annually thereafter
6through17
The extent to which a child is at risk for the development of eye and vision problems determines the appropriate re-evaluation schedule. Children with ocular signs and symptoms require a prompt, comprehensive examination. Furthermore, the presence of certain risk factors may necessitate more frequent examinations based on professional judgment.
Factors placing an infant, toddler or child at significant risk for eye and vision problems include:
Prematurity, low birth weight, prolonged supplemental oxygen at birth.
Family history of myopia, amblyopia, strabismus, retinoblastoma, congenital cataracts, metabolic or genetic disease.
Infection of mother during pregnancy (e.g., rubella, toxoplasmosis, venereal disease, herpes, cytomegalovirus or human immunodeficiency virus).
Maternal smoking, use of alcohol or illicit drug use during pregnancy.
Cortical visual impairment.
Difficult or assisted labor, which may be associated with fetal distress.
High or progressive refractive error.
Strabismus.
Anisometropia.
Academic performance problems.
Known or suspected neurodevelopmental disorders.
Systemic health conditions with potential ocular manifestations.
Wearing contact lenses.
Functional vision in only one eye.
Eye surgery or previous eye injury.
Taking prescription or nonprescription drugs (e.g., over the counter medications, supplements, herbal remedies) with potential ocular side effects.
Eye exams aren’t just about vision. They’re about your health
Don’t Do Anything Visually Stressful
It’s important that you don’t overexert your eyes in the hours before your eye exam. Using digital devices, reading, driving for prolonged periods, etc can all place considerable strain on your eyes, and this means that you are more likely to suffer from eye fatigue following your eye exam. For similar reasons, you should also try and get a good amount of sleep before your eye exam. Try and schedule your appointment for the morning to make sure that your eyes are as rested as possible.
Don’t Drink Coffee
Many people start the day with a cup of coffee, but what you might not realize is that drinking caffeine can affect your blood pressure, and the more you drink, the more significant this change is likely to be. This might not seem that important, but as part of your eye exam, your eye doctor will look at the blood vessels that are found at the back of the eye. These can reflect high blood pressure and potentially cause your eye doctor to be unnecessarily concerned.
Similarly, patients should alsoavoid drinking alcohol 24 hours before their appointment if possible. Alcohol also affects your blood pressure, as well as potentially making your eyes feel dry and irritated. And this could make your tests less comfortable.
به طور كلی رنگ چشم بستگی به مقدار ماده ای به نام ملانیندارد. ملانین رنگدانه ی قهوه ای تیره است كه در عنبیه افراد وجود دارد. چشم آبی نشان دهنده میزان كم ملانین است، در حالی كه چشم قهوه ای حاوی مقدار زیادی از این ماده است. در نتیجه انسانهایی كه پوست و موی تیره دارند ، دارای مقدار زیادی ملانین هستند، بنابراین استعداد داشتن چشم قهوه ای را دارند ولی افرادی كه مو و پوست روشن دارند مقدار كمی از این رنگدانه دارند و رنگ چشم اكثر آنها روشن است.
به همین علت است كه بیشتر نوزادان با چشم آبی به دنیا می آیند ولی به مرور زمان وقتی بدن آنها شروع به تولید ملانین می كند ، رنگ چشم آنها هم عوض می شود. eResearch by Navid Ajamin -- winter 2011
وقتی كه یك انسان مقدار متفاوتی ملانین در هر یك از عنبیه هایش باشد، رنگ دو چشم او متفاوت خواهد بود.
"Heterochromia Iridium"( اصطلاح علمی برای داشتن رنگ چشم های متفاوت در یك جاندار) تقریباً در انسانها نادر ، ولی در بسیاری از حیوانات مثل اسب، گربه و بعضی از نژادهای سگ رایج است.
There are many types and causes of heterochromia. An infant can be born with it or develop it soon after birth. In these cases, it is called congenital heterochromia.
heterochromia het·ero·chro·mia -ˈkrō-mē-ə
: a difference in coloration in two anatomical structures or two parts of the same structure which are normally alike in color
In most cases, children born with heterochromia will experience no other symptoms. They do not have any other problems with their eyes or general health. However, in some cases heterochromia can be a symptom of another condition.
Causes of heterochromia in infants can include:
Horner’s syndrome
Benign heterochromia
Sturge-Weber syndrome
Waardenburg syndrome
Piebaldism
Hirschsprung disease
Bloch-Sulzberger syndrome
von Recklinghausen disease
Bourneville disease
Parry-Romberg syndrome
When a person gets heterochromia later in life, this is called acquired heterochromia.
Young Boy With Different Colored Eyes
Causes of acquired heterochromia include:
Eye injury
Bleeding in the eye
Swelling, due to iritis or uveitis
Eye surgery
Fuchs' heterochromic cyclitis
Acquired Horner’s syndrome
Glaucoma and some medications used to treat it
Latisse, a repurposed glaucoma medication used cosmetically to thicken eyelashes
Pigment dispersion syndrome
Ocular melanosis
Posner-Schlossman syndrome
Iris ectropion syndrome
Benign and malignant tumors of the iris
Diabetes mellitus
Central retinal vein occlusion
Chediak-Higashi syndrome
این خصوصیت ( داشتن دو رنگ چشم متفاوت در یك فرد) نتیجه تغییرات در یكی از ژنهایی است كه رنگ چشم را كنترل می كنند كه می تواند ارثی باشد. البته صدمات و یا بعضی از داروهای خاص در افزایش و یا كاهش مقدار رنگدانه ها در یكی از عنبیه ها تاثیر می گذارد و یا حتی بعضی از سندرم ها مانند:Syndrome Waardendurg می تواند باعث بروز این خصوصیت درفرد شود. البته درحالیكه گروهی از این افراد از لنزهای رنگی برای تطابق دو چشم خود استفاده می كنند، عده ای دیگر به این خصوصیت بارز خود می بالند!
دلیلرنگی بودن چشم
the lack of melanin causes
چشم شما به شکل کره است، که در جلو يک برآمدگی دارد و نور از همان جا وارد چشم می شود. این برجستگی را قرنيه نامند ، که بی رنگ است. پشت آن به ترتيب مردمک و عنبيه چشم قرار دارند ، که اولی بر حسب مقدار نور، فراخ يا تنگ ميشود. دومي به شکل عدسي است که شکست نور را سبب ميشود. اگر به چشم افراد مختلف نگاه کنيد، آنها را در رنگهای مختلفي خواهيد ديد . چرا در افراد مختلف رنگ چشم متفاوت است؟ در داخل عنبيه ملانين (رنگدانهها) وجود دارند همان مادهای که پوست را رنگ مي کند . سلول های کوچک ملانين قهوه ای پررنگ هستند. اگر تعداد آنها زياد باشد. رنگ چشم ها قهوه ای سير خواهد بود ، وبر عکس کم بودن آنها باعث ميشود،که چشم ها قهوه ای پررنگ باشند.
البته رنگ چشم نمي تواند به طور کامل سياه باشد ،اما دليل آبي بودن برخي چشم ها را مي توان چنين توضيح داد : چشم هايي ميتوانند آبي باشند ، که ملانين کمتری دارند . در اين گونه چشم ها توده هاي کوچکي از ماده خاصي وجود دارند، که قابل رويت نيستند آنها از هفت رنگ تشکيل دهنده نور سفيد (قرمز- نارنجي – زرد- سبز- آبي – نيلي – بنفش)،که دريافت مي کنند، همه را جذب کرده، فقط آبي را پخش مي کنند . پس رنگ آبي چشم ، بازتاب ملانين هايي است، که در عنبيه قرار دارند.
Types of eye heterochromia
The different types of heterochromia of the eye include:
Central heterochromia
Central heterochromia is characterized by having two different colors in the same iris. Usually, the outer ring of the iris is one color while the inner ring is another.
The inner ring often seems to have "spikes" of different colors that radiate from the pupil or the black circle at the center of the iris. Eyes that have this pattern may be referred to as "cat eyes." The outer color is considered to be the true iris color in people with central heterochromia.
Central heterochromia tends to occur in irises that have low levels of melanin.
Complete heterochromia
People with this condition have two different-colored eyes. For example, they may have one blue eye and one brown eye.
Sectoral heterochromia(Cat eye)
In people with sectoral heterochromia, also known as partial heterochromia, one part of the iris is a different color from the rest. Sectoral heterochromia often resembles an irregular spot on the iris of the eye and does not form a ring around the pupil.
Identifying heterochromia
Heterochromia of the eye is easy to identify. The person will have two different colored eyes or color differences within one or both eyes.
Color differences may be slight and may only become apparent under certain lighting conditions or in photographs.
Aside from variations in eye color, there are usually no other signs and symptoms of heterochromia. However, if a medical condition or trauma is responsible for the heterochromia, other signs and symptoms may be present.
A good education for your child means good schools, good teachers and good vision. Your child's eyes are constantly in use in the classroom and at play. So when his or her vision is not functioning properly, learning and participation in recreational activities will suffer.
The basic vision skills needed for school use are:
Near Vision. The ability to see clearly and comfortably at 10-13 inches.
Distance Vision. The ability to see clearly and comfortably beyond arm's reach.
Binocular coordination. The ability to use both eyes together.
Eye movement skills. The ability to aim the eyes accurately, move them smoothly across a page, and shift them quickly and accurately from one object to another.
Focusing skills. The ability to keep both eyes accurately focused at the proper distance to see clearly and to change focus quickly.
Peripheral awareness. The ability to be aware of things located to the side while looking straight ahead.
Eye/hand coordination. The ability to use the eyes and hands together[1]
Your child's vision is essential to his success in school. When his vision suffers, chances are his schoolwork does, too.
Vision problems are common among school-age kids. According to Prevent Blindness America, one in four school-age children have vision problems that, if left untreated, can affect learning ability, personality and adjustment in school.
School-age children also spend a lot of time in recreational activities that require good vision. After-school team sports or playing in the backyard aren't as fun if you can't see well.
Warning Signs of Vision Problems in Kids
Refractive errors are the most common cause of vision problems among school-age children. Parents, as well as teachers, should be aware of these 10 signs that a child's vision needs correction:
Consistently sitting too close to the TV or holding a book too close
Losing his place while reading or using a finger to guide his eyes when reading
Squinting or tilting the head to see better
Frequent eye rubbing
Sensitivity to light and/or excessive tearing
Closing one eye to read, watch TV or see better
Avoiding activities which require near vision, such as reading or homework, or distance vision, such as participating in sports or other recreational activities
Complaining of headaches or tired eyes
Avoiding using a computer, because it "hurts his eyes"
Hyperopia, also known as farsightedness, longsightedness or hypermetropia, is a defect of vision caused by an imperfection in the eye (often when the eyeball is too short or the lens cannot become round enough), causing difficulty focusing on near objects, and in extreme cases causing a sufferer to be unable to focus on objects at any distance. As an object moves toward the eye, the eye must increase its optical power to keep the image in focus on the retina. If the power of the cornea and lens is insufficient, as in hyperopia, the image will appear blurred.[1]
What does it mean to show farsightedness?
People with hyperopia can experience
blurred vision,
asthenopia,
accommodative dysfunction,
binocular dysfunction,
amblyopia, and strabismus.
Classification of hyperopia
Simple hyperopia
Pathological hyperopia
Functional hyperopia
Ornithological hyperopia
Causes
Hyperopia can be caused bysinus infections, injuries, migraines, aging or genetics.
How is farsighted vision corrected? eResearch by Navid Ajamin -- summer 2011
Farsightedness
Farsighted (also called hyperopia) is a term to describe an eye condition that lets you clearly see objects “far” or distant in your field of vision, while objects that are near appear blurry or hazy. Due to the nature of this type of vision problem, farsightedness can affect vision in different ways.
Farsightedness happens in eyes that are incorrectly focusing images behind the retina rather than directly on it. The retina is the light-sensitive tissue at the back of the human eye responsible for processing images.
Farsighted vision is treated with corrective lenses like eyeglasses or contact lenses, and can also be treated surgically with types of surgery. Farsighted vision can develop in children or adults, and between 5 and 10 percent of all Americans are considered to be farsighted.
Persons who are extremely nearsighted, have diabetes, or have had cataract surgery are also more likely to report eye floaters.
Farsightedness Symptoms
Symptoms of farsightedness include eyes that feel tired or strained, headaches, squinting and blurred vision, especially when viewing objects that are near. But symptoms can vary person to person based on the degree of farsighted vision; some may notice little visual impairment, while others may have blurred or hazy vision for objects at distance and nearby.
Farsighted vision can develop at any time, and happens in both children and adults.
Farsightedness develops when the eyeball becomes “shorter” than it should be, moving the “focal point” of the images we see from on top of the retina, to behind the retina. Abnormalities in the eye’s lens or cornea can also cause farsighted vision.
Children's eyes grow until about age 8 years. Experts say future eye disorders are translated by some signs that parents should be careful to take measures in time. Here are some of the gestures made by children, which should give you pause for thought: eResearch by Navid Ajamin -- summer 2011
1. Approaching objects.When the baby tends to close the sheet on which color, of the eye, reduce eye to see better, you tend to approach toys to have fun better then very likely shows thetype of vision disorders myopia. 2. The distance of objects by the eye.At the opposite pole lies the distant behavior of objects, which demonstrates a pathology of type-sighted eye, that sees little better at long distances, but it almost look more tired and not well seen. This type of pathology is very rare at young age.
3. Crying in certain situations.If your child cries when objects are brought close to the eye or if he feels uncomfortable when they watch TV, could have an eye problem.
4. When your child fears of light.When your child becomes sensitive to light, even close his eyes, it is advisable to go at an ophthalmologist.
5. Playing with his eyes.If your child plays with crossed his eyes may squint and look at young age and it is still correct.If he rub his eyes often-tired very likely to. If he her his eyes should weep often go with him at an ophthalmologist to learn about the causes of irritation. They often have red eyes.Excessive blinking can hide pathologies of the conjunctiva, excessive dryness of it. If your child has frequently accused dizziness or headaches, the cause may be due to eye fatigue.
WHAT IS A CATARACT (CAT-ah-rackt)? The word cataract is derived from a Greek word meaning "waterfall" (looking through falling water). Cataracts are most commonly caused by chemical changes within the lens of the eye, which is thought to be part of the natural aging process.[1]
A cataractis a gradual clouding of the eye's natural lens. The formation of a cataract occurs during the normal process of aging. Although cataracts may affect people of any age, they are most common in older adults. Because cataracts form gradually, the symptoms are often difficult to spot. Perhaps you have noticed increased difficulty when driving toward the sun, find it harder to see traffic lights against a bright sky, or find it takes longer for your vision to return to normal after passing an oncoming set of bright headlights.
Symptoms include reduced depth perception, diminished color perception, annoying glare in sunlight, and poor night vision. Headaches, eye fatigue, burning, and watering of the eyes when exposed to bright light are also some other symptoms attributed to cataracts.[2]
More than half of all Americans age 65 and older have cataracts.
What Causes Cataracts?
The eye functions much like a camera. Light rays enter the eye, passing through the cornea, the aqueous humor -- transparent fluid in the front of the eye -- and then the pupil and into the lens. The lens bends the light rays to focus objects onto the retina lining the back of the eye. From there, the image passes through the retinal cells, into the optic nerve, and finally to the back of the brain which process the images.
Cataracts occurwhen there is a buildup of protein in the lens that makes it cloudy. This prevents light from passing clearly through a the lens, causing some loss of vision. Since new lens cells form on the outside of the lens, all the older cells are compacted into the center of the lens resulting in the cataract.
Types of cataracts include:
Age-related cataracts. As the name suggests, this type of cataract develops as a result of aging.
Congenital cataracts. Babies are sometimes born with cataracts as a result of an infection, injury, or poor development before they were born, or they may develop during childhood.
Secondarycataracts. These develop as a result of other medical conditions, like diabetes, or exposure to toxic substances, certain drugs (such as corticosteroids or diuretics), ultraviolet light, or radiation.
Traumatic cataracts. These form after injury to the eye.
Other factors that can increase a person's risk of developing cataracts include cigarette smoke, air pollution, and heavy alcohol consumption.
What Are the Symptoms of Cataracts?
Cataracts usually form slowly and cause few symptoms until they noticeable block light. When symptoms are present, they can include:
Vision that is cloudy, blurry, foggy, or filmy.
Progressive nearsightedness in older people often called "second sight" because they may no longer need glasses.
Changes in the way you see color because the discolored lens acts as a filter.
Problems driving at night such as glare from oncoming headlights.
Good eye sightis an important part of a child's overall health and development. Children who see better are more likely to do well in school and have reading confidence. Poor eye sight can have many causes and is often treatable if detected early. Since children may not be able to communicate eye problems, care should be taken to help detect poor eye sight in children.
Instructions
Schedule regular eye exams. Children should begin receiving complete eye exams at the age of six months for early detection of vision problems. The doctor will preform age appropriate tests to check for a variety of structural or functional vision problems.
Listen for complaints of tired eyes or headaches. Many children can not explain the specific pain or problem being experienced. These complaints could indicate eye strain and may be cause for a check up.
Assess whether the child is rubbing his eyes excessively. This could indicate the child's vision is not clear and needs to be focused with corrective measures.
Note whether the child has sensitivity to light. This can be observed by watching for squinting or excessive tearing when entering bright areas. The child may also shield her eyes from bright lights as a defensive measure.
Observe how close the child sits to the television. Sitting too close to the television could indicate the child is struggling to make out the images. This also applies to activities involving reading.
Watch for falling grades and decreased motivation to read. Poor eye sight in children can lead to falling grades by making it harder for the child to concentrate or even follow his reading assignments. The child may become frustrated by his inability to see words correctly or fear being ridiculed by her peers.
Blinking, a normal involuntary reflex, occurs, on average, 12 times per minute or 17,000 times a day, Professor Alan Hedge of Cornell University states. Sometimes children begin blinking so frequently it seems that they're blinking 17,000 times a minute, rather than a day. Parents often get concerned over the causes of rapid eye blinking, but most blinking is benign and self-limiting, according to a 2001 study reported by lead author David Coats of Baylor College of Medicine in the journal "Ophthalmology."
Causes
Causes for frequent blinking vary greatly. Frequent blinking can occur because a child has visual problems such as convergence insufficiency, which is troublefocusing both eyes on an up-close object. Double or blurred vision caused by convergence insufficiency can lead to excessive blinking, Baylor College of Medicine explains. Problems with the eyelids or the anterior segment of the eye, which consists of the cornea, iris, anterior chamber and lens, accounted for 37 percent of excessive blinking, Coats reported in the 2001 "Ophthalmology" study. Uncorrected refractive errors caused 14 percent of cases, he added.
Habit tics accounted for 23 percent of excessive blinking in Coats' report. Tics may also occur in children with Tourette's syndrome, a type of tic disorder that usually begins between ages 3 and 10, Family doctor.org reports. Movement disorders, called dystonias, can also cause excessive blinking, the National Institute of Neurological Disorders and Stroke reports. Allergic reactions can also cause excessive blinking, pediatrician Jeffrey Hull states. Rapid eye blinking may also occur as part of epilepsy, notes the Milton S. Hershey Medical Center.
Excessive Blinking in Children
Characteristics
In 89 percent of children with excessive blinking, both eyes are affected. Boys with excessive blinking outnumber girls two to one, Coats reported.
Diagnosis
History and clinical examination are usually adequate to make a diagnosis, Coats says, with neurological examination and neuroimaging usually not being required.
Treatment
Treatment depends on the cause. Tics often require nothing more than ignoring the symptoms until they disappear, Hull advises. Medications may help relieve specific symptoms of Tourette's. Correcting refractive errors and vision problems helps stop blinking caused by trouble seeing. Anticonvulsants are used to treat epilepsy. Dystonias may also respond to medications such as anticonvulsants as well as drugs that correct neurotransmitter abnormalities.
Considerations
?Why Is My Toddler Blinking a Lot
Excessive blinking rarely causes serious problems and often resolves without treatment. Blepharospasm, a type of dystonia that causes first one eye and then both, in most cases, to close forcefully and repeatedly, can cause functional blindness even though both eyes see normally, by causing the eyelids to eventually remain completely closed, the National Institute of Neurological Disorders and Stroke warns. Conditions such as epilepsy and dystonia require close medical evaluation and follow-up.eResearch by Navid Ajamin -- spring 2011
Excessive blinking can be caused by problems with the eyelids or anterior segment (front surface of the eye), habitual tics, refractive error (need for glasses), intermittent exotropia or turning out of the eye, and stress. It is very rare for excessive blinking to be a sign of an undiagnosed neurologic disorder.
A pediatric ophthalmologist will be able to diagnose the cause of the symptoms. A thorough exam will be performed. If there is a problem such as an ingrown eyelash, corneal abrasion (scratch on the front surface of the eye), conjunctivitis (pink eye), foreign body in the eye, allergies affecting the eye or eye dryness, this can easily be diagnosed by performing an examination with an instrument called a slit lamp. This is a special microscope used to magnify the eye. If glasses are needed, this can also be easily detected. Any strabismus (in turning or out turning of the eye) will be diagnosed when the ophthalmologist examines the eye movements.
A pediatric ophthalmologist will be able to diagnose the cause of the symptoms. A thorough exam will be performed. If there is a problem such as an ingrown eyelash, corneal abrasion (scratch on the front surface of the eye), conjunctivitis (pink eye), foreign body in the eye, allergies affecting the eye or eye dryness, this can easily be diagnosed by performing an examination with an instrument called a slit lamp. This is a special microscope used to magnify the eye. If glasses are needed, this can also be easily detected. Any strabismus (in turning or out turning of the eye) will be diagnosed when the ophthalmologist examines the eye movements.If an abrasion or conjunctivitis is diagnosed, eye drops, or ointment may be given.
Glasses may be prescribed if the excessive blinking is caused by blurry vision.
بلفارواسپاسم Blepharospasmبه معنای پلک زدن غیر ارادی یا بسته شدن غیر ارادی پلکها است.
بلفارواسپاسم یک عارضه پیش رونده عصبی است که بیشتر در زنان میانسال و سالمند اتفاق میافتد.
علت ایجاد بلفارواسپاسم چیست؟
به نظر می رسد كه بلفارواسپاسم ناشی از نوعی از اشكال در عملكرد “عقدههای قاعده ای مغز” باشد. عقده های قاعده ای بخشی از مغز هستند كه در تنظیم حركات هماهنگ عضلات دخالت دارند. البته هنوز به طور دقیق نمی دانیم كه چه مشكلی باعث بروز بلفارواسپاسم می شود.
در بیشتر موارد بلفارواسپاسم به صورت خودبهخودی و بدون هیچ علت مشخصی ایجاد می شود.
البته در بسیاری از افراد، خشكی چشم عامل محركی باشد كه در افراد حساس باعث شروع بلفارواسپاسم شود.
گاهی بلفارواسپاسم یا انواع دیگر دیستونی در افراد یك خانواده بروز می كند، بنابراین شاید زمینه های ارثی و ژنتیكی در بروز آن مؤثر باشند.
توصیههای بیماری بلفارواسپاسم [3]
۱. آموزش بیمار و اطرافیان و حمایت موثر افراد خانواده از فرد مبتلا به بلفارواسپاسم میتواند نتایج مفیدی در کنترل علائم داشته باشد.
۲. استفاده از عینکهای آفتابی تیره به دو علت به مبتلایان بلفارواسپاسم کمک میکند. اول آنکه عینک آفتابی با جلوگیری از تابش نور شدید به چشم، مانع از تحریک چشم شده و تا حدی از بروز حمله بلفارواسپاسم جلوگیری میکند.
ثانیاً عینک تیره با پنهان کردن چشم، مانع از آن میشود که سایرین متوجه پلک زدن غیر عادی فرد شوند، در نتیجه حضور در اجتماع را برای فرد آسانتر میکند.
۳. استفاده از قطرههای اشک مصنوعی و مرطوب کنندههای چشم برای درمان خشکی چشم و درمان التهاب پلک (بلفاریت) با کاهش تحریک سطح چشم ممکن است به کنترل حملات بلفارواسپاسم کمک کند.
?Why do we blink so much
لرزش پلک چشم چیست؟ [4]
لرزش چشم یا پرش پلک که با نام میوکیمیا نیز شناخته می شود، یکی از اسپاسم های ناخواسته عضلات پلک چشم است که معمولا در پلک بالا رخ می دهد، البته میوکیمیا ممکن است در پلک پایین هم رخ دهد. در این حالت پلک چشم می پرد و ممکن است این حرکت آنقدر خفیف باشد که شخص متوجه آن نشود و در حالتی دیگر نیز ممکن است آنقدر لرزش پلک چشم شدید باشد که باعث کلافه شدن فرد شود. دلیل عمده این نوع پرش ها، انقباضات غیر ارادی ماهیچه ها است که با روش هایی می توان از این انقباضات ماهیچه ای جلوگیری کرد.
دلایل
همانگونه که گفته شد، لرزش های پلک چشم معمولا به دلیل اسپاسم های عضلات چشم و پلک است که این اسپاسم ها می تواند به دلایل ذیل رخ دهند.
خستگی و سوزش چشم ها
کشیدگی عضلات اطراف چشم
کارهای سنگین فیزیکی
میزان استرس بالا
مصرف برخی از داروها
مصرف کافئین، تنباکو و الکل? pet allergens -- Does allergies cause blinking
در واقع موارد ذکر شده می توانند در بوجود آمدن و تشدید اسپاسم های عضلانی پلک بسیار موثر باشند. اما به جز موارد گفته شده،دلایل عصبی و مغزی دیگری نیز وجود دارند که باعث ایجاد عارضه پریدن پلک می شوند که این دلایل عبارتند از:
فلج صورت یکی از مشکلاتی است که ممکن است باعث لرزش غیر طبیعی پلک شود.
دیستونی که یکی از عواملی است که باعث ایجاد اسپاسم ناگهانی عضلات می شود.
بیماری پارکینسون می تواند منجر به لرزش پلک های چشم شود.
سندرم تورتس نیز می تواند باعث حرکت های ناخواسته و پرش پلک شود.
خراش های موجود بر روی قرنیه چشم نیز ممکن است باعث پرش پلک شود.
بیماری سیستم عصبی موسوم به مولتیپل اسکلروز نیز می تواند منجر به اختلالات حرکتی در پلک ها شود.
برای درمان لرزش پلک چشم، ابتدا باید عاملی که در به وجود آمدن لرزش پلک تاثیر داشته است را شناسایی کرده و آن را برطرف نمایید. اما راهکارهایی وجود دارند که به صورت کلی می توانند باعث درمان این عارضه شوند.
The problem with baby’s eyes is very hard to diagnosis due to its acuteness and severity. Mainly small kids are too young to actually tell about the difference between clear vision and the blur vision. Normally when kids reach an age of 4 years or so, their parents must be constantly looking out for such signs.
Normally there are some telltale signs which tell much about the presence of baby eyes problem but they are not that evident in toddlers and babies eyes.
According to a recent research, as many as 20 percent of kids at an age of 3 to 5 years are more prone to eye problems and parents need to pay attention towards this element. If this is ignored at that age, it can lead to more problems later on. It is therefore necessary to get a vision screening of kids every six months. Apart from this screening, there are some other things which parents can do to solve baby eyes issue.
Baby eyes problem are either due to congenital issues or acquired. Congenital occurs due to developmental issues. When damage is due to the intrauterine development after an intake of any drugs by mother or some infections. Mothers with congenital problems have no symptom common. On the other hand in the case of acquired baby eyes problem starts in the initial 28 days of baby’s life. This is normally infective since origin.
It is always pretty easy for parents to find out the presence of baby eyes problem.
Farsightedness: in this case the distinct objects appear clear to babies while they feel problem when focusing on close things. Kids mainly rub their eyes more often and try to sit closer to television. At times they even squint to make their vision clear. When doing some work, like drawing or reading, kid may not be able to stay focused for a longer period of time. The extreme farsightedness causes inability to view even the far end things. Naturally new babies are born with some signs of farsightedness but with the passage of time, their eyes are adjusted to normal view. If fail to treat, it can have drastic effects on the baby eyes.
The nearsightedness is associated with an ability to see near objects while difficulty in focusing the far ends things. Such kids squint when view near objects and also complain of an inability to see chalkboard in school from far distance. Either a child is given spectacles or making him sit in the front row can also resolve problem. If the both eyes of a baby are even, kids of age 4 years or so are not given spectacles, however in case of strain problem has to be identified to avoid further problems.
The last problem that baby eyes may get is astigmatism, but this can only be diagnosed by professional as layman can’t figure out
How Can I Tell if My Child Has Myopia
It is always better to take babies to pediatric if you feel any problem with their eyes.
Amblyopia (Lazy Eye)
Amblyopia, also known as lazy eye, is a condition in which one or both eyes do not develop normal vision due to various factors that cause the visual part of the brain to function abnormally. This weakens the eye and can lead to long-term vision problems. If recognized early, amblyopia generally responds well to treatment. Amblyopia therapy can include glasses, patching, eye drops, and sometimes surgery. Click here to learn more about amblyopia.
Astigmatism-Farsightedness-Nearsightedness
These three conditions, or refractive errors, are the most common eye problems in children and adults and are most often caused by abnormalities in the surface of the eye that prevent light from properly being focused on the retina. Click here to learn more about these refractive errors.
Childhood Tearing/Epiphora
Epiphora is the term for excessive tearing. Childhood epiphora is often noted soon after birth, but can be acquired later. When noted during infancy, it is usually due to blockage of the tear drainage system. This type of tearing often improves spontaneously by 6 to 12 months of age. Medical treatment includes tear sac massage and eye drops, but if tearing persists, surgical probing of the drainage system may be required. Other rare causes of childhood tearing include pediatric glaucoma and ocular surface diseases.
Cortical Visual Impairment
Cortical visual impairment (CVI) is vision loss due to any abnormality of the visual center in the brain. The eyes are normal, but the visual interpretation center in the brain does not function properly and prevents normal vision.
Developmental Abnormalities
During development of the fetus, abnormalities in the visual system can occur. Some developmental abnormalities include coloboma, microphthalmia (small eye), and optic nerve hypoplasia. These abnormalities often result in vision loss.
Double Vision
Double vision (diplopia) is typically caused by misalignment of the eyes (strabismus), which causes one to see an object in two different places at the same time. The object can be displaced in a horizontal, vertical, or diagonal fashion. Double vision can result from many conditions and should be evaluated at the time of onset. Treatment for double vision can include prism glasses, strabismus surgery, or Botox injections.
Genetic Eye Disease
Many eye diseases have a known genetic abnormality. These diseases are often inherited and frequently there are other family members who have had the disease. In cases of known inherited eye disease in the family, early evaluation is important. The Dean McGee Eye Institute has an ophthalmic genetic counselor who routinely sees patients in the clinic.
Nystagmus
Nystagmus is an involuntary, rhythmic oscillation of the eyes. The eye movements can be side-to-side, up and down, or rotary. Nystagmus may be present at birth or acquired later in life. It may result from abnormal binocular fixation early in life, and may also accompany a number of eye disorders and neurological diseases.
Pediatric Cataract
A cataract is a cloudiness or opacification of the normally clear lens of the eye. Depending on the size and location, the cataract can interfere with light passing to the retina and cause blurred vision. Cataracts are typically associated with older adults, but cataracts can occur at birth or during childhood. Early detection and treatment of cataracts are critical in infants and young children in order to restore normal visual development. A white area in the pupil and misalignment of the eye can be a sign of cataract.
Pediatric cataracts that significantly obstruct vision require surgery. Patients subsequently require treatment with eyeglasses, bifocals, or contact lenses, and eye-patching. Often, pediatric cataracts result in some degree of lazy eye (amblyopia) and strabismus as well.
Pediatric Glaucoma
Glaucoma is a condition that is associated with high pressure within the eye. This pressure can damage the optic nerve, which is critical for vision, resulting in permanent vision loss. Pediatric glaucoma is a rare condition that can present in the newborn or during childhood. Signs and symptoms of pediatric glaucoma include cloudy corneas, tearing, frequent blinking, light sensitivity, and redness of the eye.
Pediatric Ptosis (Drooping Eyelid)
Ptosis, or drooping of the upper eyelid, occurs in both children and adults. Children can be born with ptosis (congenital) or acquire it during childhood. Neurological diseases can also trigger it.
Ptosis is caused by weakness in the muscle that elevates the eyelid. A droopy eyelid can block light passing to the retina in the back of the eye and/or create significant astigmatism that produces a blurry image in the affected eye. These situations cause lazy eye (amblyopia) and, if untreated, can result in permanent loss of vision. In addition, children may develop a chin-up head position due to the droopy eyelid. If the ptosis is significant, surgical correction may be necessary.
Retinopathy of Prematurity (ROP)
Retinopathy of prematurity (ROP) is an eye disease that occurs in some premature infants. It results from abnormal development of the blood vessels in the retina. ROP is progressive, starting with mild changes and sometimes progressing to severe, sight-threatening changes. Most infants with ROP improve spontaneously, but some develop severe changes that require laser treatment or injections of medicine into the eye.
Complications of ROP can include strabismus (eye misalignment), myopia (nearsightedness), cataract, and, in severe cases, blindness from retinal detachment. Premature infants at risk of ROP are identified in the hospital and enrolled in a routine screening protocol.
Strabismus (Crossed Eyes)
Strabismus is the term for misalignment of the eyes in which an eye may be turned inward, outward, upward, or downward. Strabismus in children can result in lazy eye (amblyopia) and cause permanent loss of vision if treatment is delayed. Adults and older children often experience double vision (diplopia). Depending on the type and cause of the strabismus, treatment may include eyeglasses, prisms, surgery, Botox injection, or eye-patching therapy.
If you can see objects nearby with no problem, but readingroad signsor making out the writing on the board at school is more difficult, you may be near- or short-sighted.
Your eye care professional may refer to the condition as myopia, a term that comes from a Greek word meaning "closed eyes." Use of the word "myopia" for this condition may have grown out of one of the main indications of nearsightedness: Squinting to see distant objects clearly.
Myopia is not a disease, nor does it mean that you have "bad eyes." It simply refers to a variation in the shape of your eyeball. The degree of variation determines whether you will need corrective eyewear.
What causes nearsightedness ?Myopia most often occurs because the eyeball is too long, rather than the normal, more rounded shape. Another less frequent cause of myopia is that the cornea, the eye's clear outer window, is too curved. There is some evidence that nearsightedness may also be caused by too much close vision work.
How does myopia affect sight ?Our ability to "see" starts when light enters the eye through the cornea.
The shape of the cornea, lens and eyeball help bend (refract) light rays in such amanner that light is focused into a point precisely on the retina. In contrast, if you are nearsighted, the light rays from a distant point are focused at a place in front of the retina. As the light will only be focused in that one place, by the time it reaches the retina it will have "defocused" again, forming a blurred image.
Who is affected by nearsightedness ?Myopia usually occurs between the ages of 8 to 12 years. Since the eyes continue to grow during childhood, nearsightedness usually occurs before the age of 20. Often the degree of myopia increases as the body grows rapidly,then levels off in adulthood.
During the years of rapid growth, frequent changes in prescription eyewear may be needed to maintain clear vision.
How is myopia diagnosed ?Myopia is often suspected when a teacher notices a child squinting to see a blackboard or a child performs poorly during a routine eye screening. Further examination will reveal the degree of the problem. A comprehensive eye health examination will detect myopia. Periodic examinations should follow after myopia has been discovered to determine whether the condition is changing, and whether a change in prescriptive eyewear is needed. Eye exams also help to ensure that vision impairments do not interfere with daily activities.
How is myopia treated ?
Corrective concave lenses are prescribed to help focus light more precisely on the retina, where a clear image will be formed. Depending on the degree of myopia, glasses or contact lenses may be needed all of the time for clear vision. If the degree of impairment is slight, corrective lenses may be needed only for activities that require distance vision, such as driving, watching TV or in sports requiring fine vision.
How will nearsightedness affect my lifestyle ?
If glasses or contact lenses are prescribed, it may take you a few days to adjust to them. After that, nearsightedness will probably not significantly affect your lifestyle. However, more severely nearsighted individuals may find the condition limits their choice of occupation in some cases.
Nearsightedness in children
School age children may have vision problems ranging from mild to severe. When problems are suspected, it is important that the child have a comprehensive eye health examination to determine the nature of the problem and to rule out serious eye diseases. When vision conditions are treated properly, the child will enjoy the best possible sight.
To help a child cope with nearsightedness
- Avoid referring to the child's eyes as "bad eyes;" instead tell the child that his or her eyes just bend light differently and corrective lenses are needed to help focus light rays.
- Use illustrations and simple explanations to help the child understand how a differently-shaped eyeball may result in his or her being nearsighted.
- Make the occasion of selecting new frames for lenses a fun time.
- Consider contact lenses as an option.
- Do not restrict the child's activities because of poor vision.
- Include the child in discussions about his or her eyesight.
Encourage the child to verbalise concerns about the adjustment to rapidly changing vision.
سيستم بينايي در بدو تولد يك سيستم تكامل نيافته است و تكامل آن در طول سال اول زندگي رخ مي دهد. از اين رو، توجه والدين و پزشكان به مشكلات احتمالي در طول سال اول نقشي بسيار تعيين كننده در تكامل بينايي كودك و جلوگيري از مشكلات ناشي از اختلال در بينايي نظير مشكلات يادگيري خواهد داشت.
سه ماه اول نوزادان معمولا قبل از هر چيز “حركت” را مي بينند. نوزاداني كه به موقع بدنيا آمده باشند (هفته ۳۸ تا ۴۲ حاملگي) بايد بتوانند تغييرات صورت مادر نظير خنده، اخم، … را در هفته اول بعد از تولد ببينند. در اين زمان درك رنگ هنوز كاملا تكامل نيافته و درك عمق نيز در طول سال اول به موازات هماهنگ شدن حركت چشم ها ايجاد مي شود. هماهنگي عضلات چشم در نوزادان تازه متولد شده و شيرخواران بسيار ناقص است. چشم نوزادان اغلب به بيرون يا داخل منحرف شده و حركت چشم ها با هم هماهنگ نيست. اين وضعيت استرابيسم يا انحراف چشم خوانده مي شود. اگر استرابيسم تا ۳ يا ۴ ماهگي خودبخود بر طرف نشود بهتر است نوزاد توسط يك چشم پزشك معاينه شود.
اولين علائم مشكلات چشم و بينايي در بعضي موارد لازم است نوزاد قبل از ۳-۴ ماهگي مورد معاينه قرار گيرد. اين موارد عبارتند از: انحراف شديد چشم ها، عدم حركت چشم قبل از ۳ ماهگي، انحراف هر دو چشم به داخل، ثابت ماندن يك چشم در زمان حركت چشم ديگر و يا تفاوت فاحش بين حركات دو چشم. تشخيص زودرس استرابيسم بسيار مهم است زيرا تنبلي چشم يا آمبليوپي حاصل استرابيسم درمان نشده است. اگر يك چشم كودك نتواند بر اثر استرابيسم خوب ببيند هماهنگي چشم ها بر هم مي خورد. همچنين اگر مغز تصويري از يكي از چشم ها دريافت نكند در طول زمان علائم ارسالي از چشم مبتلا را ناديده مي گيرد و نهايتاً فرد دچار تنبلي چشم و متعاقب آن كاهش شديد ديد مي شود.
مشكلات بينايي در نوزادان نارس تكامل بينايي در نوزادان نارس كمي بيشتر از نوزاداني كه به موقع بدنيا آمده باشند طول مي كشد. احتمال ايجاد استرابيسم و آمبليوپي در نوزاداني كه قبل از هفته ۳۵ حاملگي بدنيا آمده باشند ۳۰% بيشتر است. هر چه نوزاد زودتر از زمان طبيعي بدنيا بيايد اين احتمال افزايش مي يابد. نوزاد بايد كاملا به نور روشن (مثلا لامپ) و يا آويز هايي كه معمولا بالاي سر نوزادان آويزان مي كنند توجه كند. اگر در ۳ ماهگي جسم را جلو چشم نوزاد بگيريد و آن را از يك سمت آهسته به سمت ديگر ببريد و نوزاد قادر به دنبال كردن آن با چشم نباشد بهتر است مورد معاينه قرار گيرد. البته در بعضي موارد تكامل بينايي ديرتر رخ مي دهد كه به آن تأخير در تكامل بينايي مي گويند.
حركات نامنظم چشم اختلالي بنام نيستاگموس ممكن است در نوزادي رخ دهد. در اين اختلال چشم ها حركاتي به چپ و راست، حركات دوراني و يا حركات نامنظمي دارند. علت اين اختلال ممكن است ضعف بينايي، وجود نقص در مسير عصبي از چشم به مغز و يا آلبينيسم (كمبود رنگدانه ها) باشد. نيستاگموس ممكن است ارثي هم باشد. نوزاداني كه نيستاگموس دارند ممكن است ديد طبيعي و يا ضعيف داشته باشند. اگر نيستاگموس تا بعد از ۳ ماهگي باقي بماند نوزاد بايد مورد معاينه قرار گيرد. در مجموع بايد گفت كه ۳ تا ۴ ماه اول زندگي زمان بسيار مهمي از نظر تكامل بينايي است و توجه والدين و مراجعه به موقع به چشم پزشك نقش تعيين كننده اي در بينايي كودك خواهد داشت.
۴ تا ۶ ماهگي در اين سن نوزاد بايد دستش را به طرف اسباب بازي كه جلوي او مي گيريد دراز كند و يا دستش را به آن بزند. در ابتدا ممكن است دست نوزاد بطور اتفاقي به جسمي كه جلويش گرفته ايد بخورد ولي در طول زمان با رشد بينايي، درك عمق و درك بيشتر نوزاد اين كار ارادي تر مي شود. از ۶ تا ۸ ماهگي نوزاد شروع به غلت زدن و احتمالا چهار دست و پا راه رفتن مي كند. در اين مرحله مي توانيد يك اسباب بازي را طوري جلو كودك قرار دهيد كه مجبور باشد براي رسيدن به آن غلت بزند و يا كمي از جاي خود جلوتر بيايد. اين كار به تقويت بينايي نوزاد كمك مي كند.
بين ۸ تا ۱۲ ماهگي
نوزاد شما ممكن است چهار دست و پا حركت كند و يا راه برود. سعي كنيد به جاي راه افتادن زودتر، كودك خود را به حركت چهار دست و پا تشويق كنيد زيرا باعث ايجاد هماهنگي ميان حركات دست و چشم مي شود. در اين سنين بويژه وقتي كودك روي مبل يا تخت و يا نزديك پله است بايد بسيار مواظب وي بود زيرا ديد كودك در اين مرحله هنوز فاقد درك عمق كافي است و در نتيجه پستي و بلندي ها را بخوبي درك نمي كند. به عبارت ديگر كودك در اين سن متوجه نيست كه لبه تخت در جايي تمام مي شود و زمين پايين تر از آن قرار گرفته است بنابراين احتمال سقوط كودك از تخت و پله وجود دارد.
تنبلي چشم نوعي اختلال بينايي است كه اگر به موقع تشخيص داده و درمان نشود ، فرد را از يك چشم بسيار كم بينا يا نابينا مي كند و با تشخيص به موقع ، به راحتي و كاملا قابل درمان است.
چشمان برخي كودكان ، با آنكه سالم به نظر مي رسند اما از سلامتي و ديد كافي برخوردار نيستند . رشد و تكامل مركز بينايي در مغز از دوران جنيني تا حدود ده سالگي ادامه دارد ، اما حداكثر سرعت رشد آن تا سه سالگي است .
Classification and Types
Stimulus deprivation or amblyopia of disuse
Amblyopia secondary to nystagmus
Anisometropic amblyopia
Isoametropic amblyopia
Strabismic amblyopia
Meridional amblyopia
Idiopathic amblyopia
Organice amblyopia
نتيجه تكامل دستگاه بينايي ، در اين دوران ، ديد واضح و كامل است . در اين مدت ، بخصوص در سه سال اول زندگي ، هر عاملي كه باعث اشكال ديد ، در يك يا هر دو چشم كودك شود ، رشد و تكامل دستگاه بينايي را متوقف مي سازد و در نتيجه باعث كاهش ميزان بينايي طفل مي شود . معني اين سخن آن است كه امكان دارد چشمي را كه از نظر ظاهر كاملا طيعي است از بينايي كامل و طبيعي برخوردار نباشد. در صورتي كه اشكال ديد كودك ، قبل از پنج سالگي درمان شود ، حتي اگر چشم در اين مدت تنبل شده باشد با درمان ، بينايي كامل بدست مي آيد . پس از پنج سالگي ، هر چه درمان چشم تنبل بيشتر به عقب بيافتد ، احتمال به دست آوردن بينايي كامل كمتر مي شود . به طوري كه پس از هفت تا ده سالگي ، درمان هيچ تاثيري در بينايي نخواهد داشت. آمبليوپينوعي كاهش بينايي است كه در ان نمي توان در چشم و يا در راههاي عصبي بينايي هيچ گونه عيب ارگانيك (ساختماني)واضحي براي آن يافت و در واقع از مواردي است كه نه مريض چيزي مي بيند ونه دكتر در چشم مريض چيزي مي بيند از نقطه نظر باليني زماني تشخيص آمبليوپي مسجل مي گردد كه حتي با بهترين تصحيح انكساري نيز نتوان ديد بيمار را افزايش داد و در روي تابلوي اسنلن حداقل دو رديف اختلاف ديد وجود داشته باشد در اينجا مي توانيم بگوييم چشمي كه ديد كمتري دارد دچار آمبليوپي است با شرط اينكه در ته چشم نيز نتوان هيچ گونه ضايعه ارگانيكي كه مسئول كاهش بينايي باشد يافت نمود.
How Does Amblyopia Occur? While it is essentially the inability of the eye to focus clearly, the causes are much more detailed and widespread. According to the National Eye Institute, it is caused by a number of conditions, including:
Strabismus: The misalignment of the eyes. Strabismic amblyopia is the most frequent cause. In this situation, lazy eye occurs as a result of the brain bypassing the visual information being received from the eye that is misaligned.
Cataract: The clouding of the front part of the eye. This form of lazy eye is known as deprivation amblyopia and results from light being unable to enter and focus in the eye.
Blurry vision: Refractive error caused by the eye’s inability to focus light on the retina, often referred to as being nearsighted, farsighted, or astigmatism. This form of lazy eye is known as refractive amblyopia and occurs when the brain disregards the information being received from the eye that has the refractive error; over time, the condition develops as a result of underutilization of the weaker eye.[2]
عوامل ايجاد كننده تنبلي چشم اشكالات مادرزادي در ساختمان چشم ، مانند آب مرواريد و پايين افتادگي پلك باعث ميشود كه چشم نتواند تصوير واضحي از اشياء دريافت كند و بتدريج دچار تنبلي شود . در مورد كاتاراكت بهترين درمان عمل جراحي است كه اگر پس از تولد تا سه ماهگي هرچه سريعتر صورت بگيرد ، نتيجه بهتري خواهد داشت . اما پس از سه ماهگي نتيجه چندان رضايت بخش نخواهد بود. در نزديك بيني ، دور بيني و آستيگماتيسم ، اگر ديد هر دو چشم بسيار كم باشد ، هر دو چشم و آگر تفاوت دي آنها زياد باشد ، چشم ضعيف تر نمي تواند تصوير واضحي از اشياء دريافت كند و دچار تنبلي مي شود . لوچي يا انحراف چشم نيز مي تواند باعث دو بيني شده در نتيجه تصوير واضحي روي شبكيه تشكيل نشود . بدين ترتيب مغز بتدريج براي حذف دو بيني ، تصوير چشم منحرف را حذف كرده و تنبلي چشم ايجاد خواهد شد.
پيشگيري و درمان تنها راه پيشگيري از تنبل چشم تشخيص بموقع عوامل ايجاد كننده آن است و چون بسياري از اين عوامل براي خانواده ها ناشناخته است ، چشم همه كودكان بايد حداقل سه بار قبل از دبستان در زمانهاي مختلف معاينه شود :
سه ماهگي - دو تا سه سالگي - پنج تا شش سالگي
همچنين اگر كودكي انحراف چشم دارد ، والدين بايد به محض تشخيص ، او را نزد متخصص برده و تحت درمان قرار دهند. درمان تنبلي چشم ، معمولا با بستن چشم سالم است ، تا چشم تنبل به كار بيافتد و تنبلي آن برطرف شود . مدت بستن چشم را متخصص تعيين مي كند و در فواصل مشخص نيز بايد بوسيله متخصص معاينه شود . گاهي اوقات براي درمان عينك و در برخي موراد جراحي توصيه مي شود . اگر تنبلي چشم بر اثر بيماريهاي مادرزادي مانند آب مرواريد ، پايين افتادگي پلك يا ديگر عيوب ساختماني باشد بايد قبل از سه ماهگي درمان شود و اگر به علتهاي ديگر باشد ، درمان قطعي تا قبل از پنج سالگي امكانپذير است و بعد از آن درمان معمولا نتيجه خوبي ندارد . گاهي اوقات مدت درمات چندسال است . در اين صورت والدين طفل بايد استقامت ، پشتكار و حوصله لازم را داشته باشند و از رفت و آمد نزد متخصص و ساير مشكلات جنبي آن خسته نشوند. اگر متخصص توصيه كرد چشم كودك را ببنديد ، طبق دستور او عمل كنيد و چشم كودك را كمتر يا بيشتر از زمان تعيين شده نبنديد . در صورت تشخيص تنبلي چشم ، حتما تا پايان ده سالگي پيگير وضعيت بينايي و تغييرات عيوب انكساري كودك باشيد.[1]
Infant vision concerns the development of visual ability in human infantsfrom birth through the first years of life. The aspects of human vision which develop following birth includevisual acuity, tracking, colour perception, depth perception, andobject recognition.[1]
At birth, babies can't see as well as older children or adults. Their eyes and visual system aren't fully developed. But significant improvement occurs during the first few months of life.
Steps in Infant Vision Development
The following are some milestones to watch for in vision and child development. It is important to remember that not every child is the same and some may reach certain milestones at different ages.
Birth to four months
At birth, babies' vision is abuzz with all kinds of visual stimulation. While they may look intently at a highly contrasted target, babies have not yet developed the ability to easily tell the difference between two targets or move their eyes between the two images. Their primary focus is on objects 8 to 10 inches from their face or the distance to parent's face.
During the first months of life, the eyes start working together and vision rapidly improves. Eye-hand coordination begins to develop as the infant starts tracking moving objects with his or her eyes and reaching for them. By eight weeks, babies begin to more easily focus their eyes on the faces of a parent or other person near them.
For the first two months of life, an infant's eyes are not well coordinated and may appear to wander or to be crossed. This is usually normal. However, if an eye appears to turn in or out constantly, an evaluation is warranted.
Babies should begin to follow moving objects with their eyes and reach for things at around three months of age.
Five to eight months
During these months, control of eye movements and eye-body coordination skills continue to improve. Dep th perception, which is the ability to judge if objects are nearer or farther away than other objects, is not present at birth. It is not until around the fifth month that the eyes are capable of working together to form a three-dimensional view of the world and begin to see in depth. Although an infant's color vision is not as sensitive as an adult's, it is generally believed that babies have good color vision by five months of age. Most babies start crawling at about 8 months old, which helps further develop eye-hand-foot-body coordination. Early walkers who did minimal crawling may not learn to use their eyes together as well as babies who crawl a lot.
Nine to twelve months
At around 9 months of age, babies begin to pull themselves up to a standing position. By 10 months of age, a baby should be able to grasp objects with thumb and forefinger. By twelve months of age, most babies will be crawling and trying to walk. Parents should encourage crawling rather than early walking to help the child develop better eye-hand coordination. Babies can now judge distances fairly well and throw things with precision.
One to two years old
By two years of age, a child's eye-hand coordination and depth perception should be well developed. Children this age are highly interested in exploring their environment and in looking and listening. They recognize familiar objects and pictures in books and can scribble with crayon or pencil. [2]
What causes poor eyesight in children
Critical warning signs
Excessive tearing
Red or encrusted eyelids
White pupils
Extreme sensitivity to bright light
Constant eye turning
Vision problems
Strabismus
Nystagmus
Amblyopia
Photophobia
Tumor in the eye
Cataract [1]
Most parents or caretakers wonder whether your child needs an eye exam. Vision screenings performed by school nurses are not as complete as a comprehensive eye exam performed by an optometrist. Eye exams are extremely important for children, because vision problems are fairly common among preschoolers and school aged children. By identifying your child’s vision problems early, your child will have greater success with treatment. If left untreated, some eye conditions and diseases may stunt visual development and cause visual impairment.
According to the American Optometric Association, infants should have their first comprehensive eye exam by theage of six months. After that, children should receive additional eye exams at the age of three, and then at the age of 5 or 6. The American Optometric Association also recommends an eye exam every two years for school aged children who do not require vision correction. Children that do need glasses or contact lenses should have eye exams according to your optometrist’s recommendations.
What are common vision problems in children?
The 12 most common vision problems in children are:
Myopia (short-sighted)
Hyperopia (long-sighted)
Amblyopia (lazy eye)
Convergence Insufficiency
Depth perception and 3D vision difficulties
Double vision
Eye fatigue
Eye teaming problems
Focusing difficulties
Hand-eye coordination difficulties
Strabismus (crossed-eyes)
Visual processing dysfunction
Vision Development in Preschool and School-aged Children
Focus, tracking, depth perception, and other aspects of vision continue to develop throughout early and middle childhood. Convergence, the ability of both eyes to focus on an object simultaneously, becomes more fully developed by about age seven; this is one reason any problems a child has with focusing or eye alignment should be treated before that age.
Most children are naturally somewhat farsighted (hyperopic) but can see well at other distances. More pronounced myopia (nearsightedness) and astigmatism are thought to be inherited. There is some evidence from recent studies in the United States and Australia that the amount of time school-aged children spend outdoors, in natural light, may have some impact on whether they develop mild myopia.[3]
When scheduling an eye exam for your child, choose a time when he or she is usually alert and in a good mood. Be sure to tell us if your child has a history of delayed motor development, engages in frequent eye rubbing, fails to maintain eye contact, cannot keep visual fixation on an object, has poor eye tracking, or has failed a vision screening. We will also want to know about previous ocular diagnoses. Make sure to inform us of any family history of eye problems, such as nearsightedness, farsightedness,strabismus,amblyopia, or eye diseases.[4]
A thorough eye exam can test all of the eight vision skills needed to read. If your child is having trouble in school, it could be eyesight-related. Learn more about vision changes in school-age children. Good vision is vital to reading well. And although vision may not be the only cause of reading difficulties, it is one cause that is sometimes overlooked.
Neededto readeight vision skills Reading requires the integration of eight different vision skills. The typical school eye chart test checks only one. Quick eye examinations may cover only one or two. Since a comprehensive eye examination will cover the eight vision skills, it is a must for anyone who is having trouble reading .
The eight skills include:
Visual acuity,or the ability to see objects clearly at a distance. Visual acuity is sometimes measured in a school vision screening. Normal visual acuity is referred to as 20/20 vision (or 6/6 vision in the metric system) — a measure of what can normally be seen at a distance of 20 feet, or 6 meters. If a problem is discovered in the screening, a thorough optometric examination should follow.
Visual fixation,or the ability to aim the eyes accurately. One type of fixation, called direct fixation, has to do with the ability to focus on a stationary object or to read a line of print. The other type, called pursuit fixation, is the ability to follow a moving object with the eyes.
Accommodation,or the ability to adjust the focus of the eyes as the distance between the individual and the object being observed changes. Children frequently use this skill in the classroom as they shift focus between books and blackboards.
Binocular fusion,or the brain's ability to gather information received from each eye separately and form a single, unified image. Eyes must be precisely aligned physically or double vision may result. If it does, the brain often subconsciously suppresses or inhibits the vision in one eye to avoid confusion. That eye may then develop poorer visual acuity (amblyopia or lazy eye).
Stereopsis,a function of proper binocular fusion enhancing the perception of depth, or the relative distances of objects from the observer.
Convergence,or the ability to turn the two eyes toward each other to look at a close object. Any close work, such as desk work, requires this vision skill.
Field of vision,or the area over which vision is possible. It is important to be aware of objects on the periphery (left and right sides and up and down) as well as in the center of the field of vision.
Perception,the total process of receiving and recognizing visual stimuli. Form perception is the ability to organize and recognize visual images as specific shapes. A reader remembers the shapes of words, which are defined and recalled as reading skills are developed.
Most people don’t realize that you need17 visual skills to succeed in reading, learning, sports, and in life!
1. Eye Movement Control The ability to move both eyes together to point at an intended target or follow along a path, like a line of text
2. Simultaneous Focus at Far Forming a clear image of something in the distance
3.Sustaining Focus at Far Keeping an image of something in the distance clear
Eye chart with sports figures
4. Simultaneous Focus at Near Forming a clear image of something close to the eyes
5. Sustaining Focus at Near Keeping a clear image of something close to the eyes
6. Simultaneous Alignment at Far Lining up both eyes at the same point the distance
7. Sustaining Alignment at Far Holding both eyes lined up at the same point in the distance
8. Simultaneous Alignment at Near Lining up both eyes at the same point up close
9. Sustaining Alignment at Near Holding both eyes lined up at the same point up close
10. Central Vision (Visual Acuity) This is where "20/20" vision comes in!
11.Peripheral Vision Being able to see what's on either side of you while your eyes are pointed forward
12. Depth Awareness Being able to tell that things are further away or closer up than each other (also know as depth perception)
13. Color Perception Being able to tell different colors apart (if you are not color-blind)
14. Gross Visual-Motor Moving yourself through space without bumping into things by using information from your vision
15. Fine Visual-Motor Writing, sewing, texting, and doing other small and close-up activities with accuracy by using information from your vision
16. Visual Perception Being aware of your environment and what is going on around you in your visual field (the area you can see)
17.Visual Integration Bringing together your vision and your other senses to accomplish complex tasks, like reading while walking a balance beam
Important Vision Skills for Sports
Dynamic Visual Acuity
If you are playing a sport like racquetball, tennis, soccer or hockey, you need to be able to clearly see objects while you and/or the objects are moving fast. Without good dynamic visual acuity, you will have a difficult time in sports like these.
Visual Concentration
When you commit an error on an easy ground ball or miss a short putt, you might be distracted by things that are happening around you. Our eyes normally react to anything that happens in our field of vision-spectators, other participants or even rustling leaves on an overhanging branch. Visual concentration is the ability to screen out these distractions and stay focused on the object or the target.
Eye Tracking
When you are playing any sport with a ball or a fast-moving opponent, you need to be able to follow objects without much head motion. Eye tracking helps you maintain better balance and quickly react to the situation.
Eye-Hand-Body Coordination
Eye-hand-body coordination is how your hands, feet and body and other muscles respond to the information gathered through your eyes. It is an important part of most sports because it affects both timing and body control.
Visual Memory
When you are pushing a fast break up the basketball court, leading a rush up the ice in hockey or catching the big wave amid a crowd of surfers, you need to process and remember a fast-moving, complex picture of people and things. This is called visual memory. The athlete with good visual memory always seems to be in the right place at the right time.
Visualization
Picture yourself hitting a perfect drive ... long and right down the middle of the fairway. Believe it or not, picturing yourself doing it can actually help you do it. Through visualization, you see yourself performing well in your "mind's eye" while your eyes are concentrating on something else, usually the ball. Using scanning techniques, researchers have found that the same areas of the brain that light up during performance also are at work when you visualize the performance.
Peripheral Vision
When a soccer player sees her teammate out of the corner of her eye, she is using her peripheral vision. Much of what happens in sports does not happen directly in front of you. Therefore, increasing your ability to see action to the side without having to turn your head is important.
Visual Reaction Time
The pitcher releases the ball and you swing ... a little late and you hit a weak foul down the line, or worse, you miss the ball completely. Or maybe you can't quite return that tennis serve. You need to improve your visual reaction time, or the speed with which your brain interprets and reacts to your opponent's action.
Depth Perception
In racket sports, depth perception enables you to quickly and accurately judge the distance between yourself, the ball, your opponents, teammates, boundary lines and other objects. If you consistently over- or underestimate the distance to your target, poor depth perception may be the reason.
Is your child myopic (or nearsighted)?
Which type of myopia does your child have?
Myopia is a condition in which one can see clearly up close but unable to see clearly far away. In a myopic person, the eye is longer than it should be and so light coming into the eye from far away is focused in front of the retina rather than right on it, producing a blurred image. If the myopia starts in a child at a young age, chances are that it will worsenrapidly as the child grows.
There is actually more than one type of myopia, depending on its cause:
Infantile myopia: the child is born with high myopia, often associated with abnormal pregnancy or poor nutrition during gestation.
Stress-induced myopia: the child begins reading at a very young age and tends to be very detail-oriented. This is myopia caused by excessive near work at an age when the child ought to be spending time playing outdoors.
Myopia induced by binocular dysfunction: the child’s binocular system did not develop properly, therefore reading creates excess stress on the focusing system which in turn, induces elongation of the eye resulting in worsening eyesight.
Here are some of the many visual skills that are improved through Sports Vision Training.
Visual Acuity at All Distances (Adaptable Clear Vision) Do the two eyes maintain clear vision at varying distances at all times? Clear vision at all distances is important to sports success.
Eye Focusing Skills - Shifting and Sustaining Sharp Vision: Do the two eyes shift and sustain focusing power quickly and easily? Accurate eye focusing skills are a big boon for an athlete in any game with moving objects and/or players, especially in aVision Therapy and Sports Vision Trainingfast-paced game. Sports Vision Training can enhance focusing power, agility, and speed.
Eye Tracking, Eye Teaming, and Eye Movement Skills: Do the two eyes aim, move, and work as an effective coordinated team? Fast, fluid, binocular vision with coordinated eye movements and smooth eye tracking skills are essential to success in sports. Sports Vision Training conditions all of these visual skills simultaneously.
Depth Perception: Good binocular depth perception enables accurate assessment of relative distances, such as where the athlete's body is in relation to other objects or people. Sports Vision Training can increase and stabilize binocular depth perception.
Peripheral Vision and Awareness:Widening your peripheral field of vision and peripheral awareness allows a better perception of action, motion, space, and objects to the sides of your eyes and body without having to move your eyes in that direction. In other words, you can perceive what is happening around you without having to move your eyes away from a single focal point or visual target.Good or heightened peripheral vision and awareness add greatly to sports performance, such as in team sports. In addition, good peripheral vision contributes greatly to a well functioning vestibular system (good balance).
Of these three types of myopia, myopia induced by binocular dysfunctionis the easiest to treat with vision therapy. When a child’s eyes do not work together properly as a team, he may respond by having a performance issue in reading, or he may learn to work his focusing system extra hard in an attempt to overcome the binocular dysfunction. In such cases, treating the underlying binocular dysfunction is key to eliminating the excess strain which induced the worsening myopia to begin with.
Because the binocular dysfunction varies from person to person, we do not prescribe the same vision therapy exercises for myopia control to all patients. There are many programs for natural vision improvement out there, but we don't typically recommend them because they are not customized to address each individual patient's binocular problems.
? What are Visual Skills
For stress-induced myopia, vision therapy may be helpful but it requires constant vigilance and continual therapy. Patients will need to learn drills to reduce the stress on their eyes, learn proper posture and improve visual hygiene. In addition, plus lenses may be prescribed to further decrease the stress on their eyes when reading. For such patients, orthokeratology, an overnight contact lens which reshapes the eye while sleeping, tends to work better in arresting the worsening of their eyesight.
There are several key visual skills that are enhanced through sports vision programs for athletes that aim to achieve their optimal sports performance, these include: Dynamic visual acuity: this refers to the patient’s ability to see objects clearly while in motion. This is exceptionally important as hand-eye coordination and reflex reactions are essential for success in most sporting activities. Contrast sensitivity: good contrast sensitivity is needed to determine the difference between an object and its surroundings. Contrast sensitivity is particularly important in situations where there may be low light, fog or glare that could diminish the natural contrast between objects and backgrounds. Eye tracking: this refers to the ability to follow a fast-moving object, such as a ball or puck. Switching eye focus: athletes need to be able to change their focus quickly and accurately from one distance to another. Binocular vision skills: also known as eye teaming skills, these skills determine how well your eyes work with one another to produce a single, clear image.
Processing speed: visual processing speed is defined as the amount of time it takes to make a correct judgement about a visual stimulus – for example, how fast a ball is travelling towards them. Peripheral awareness: athletes also need to be able to be aware of what is happening at the edges of their vision while also concentrating on a fixed object in front of them.
Sports vision testing can enable your eye doctor to spot any weaknesses that you may have in any of these key visual skills. By identifying them, it is possible for you to undergo treatment to overcome theses issues and meet your specific goals that will ultimately enhance your overall athletic performance. This is known as sports vision training.
وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.


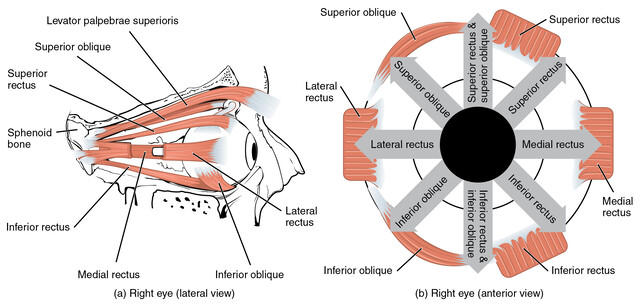

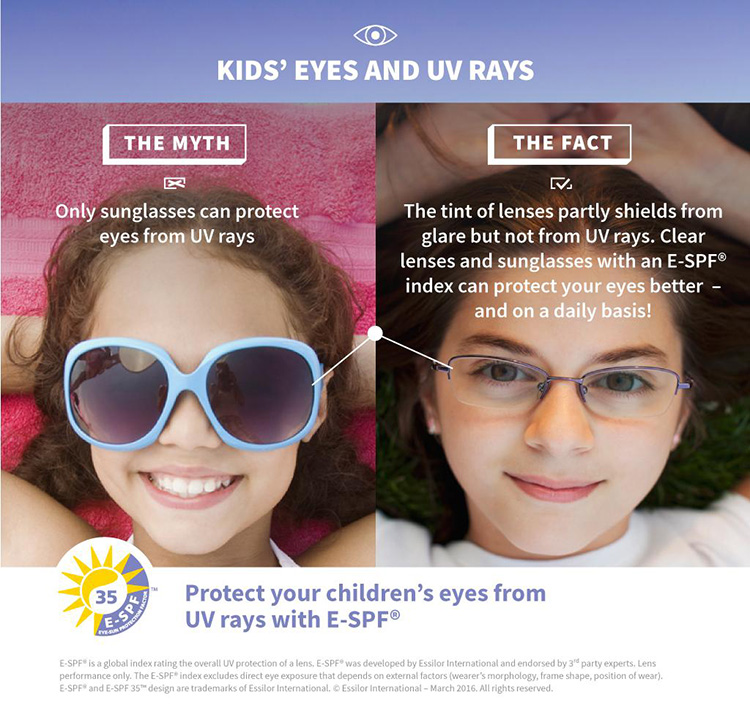


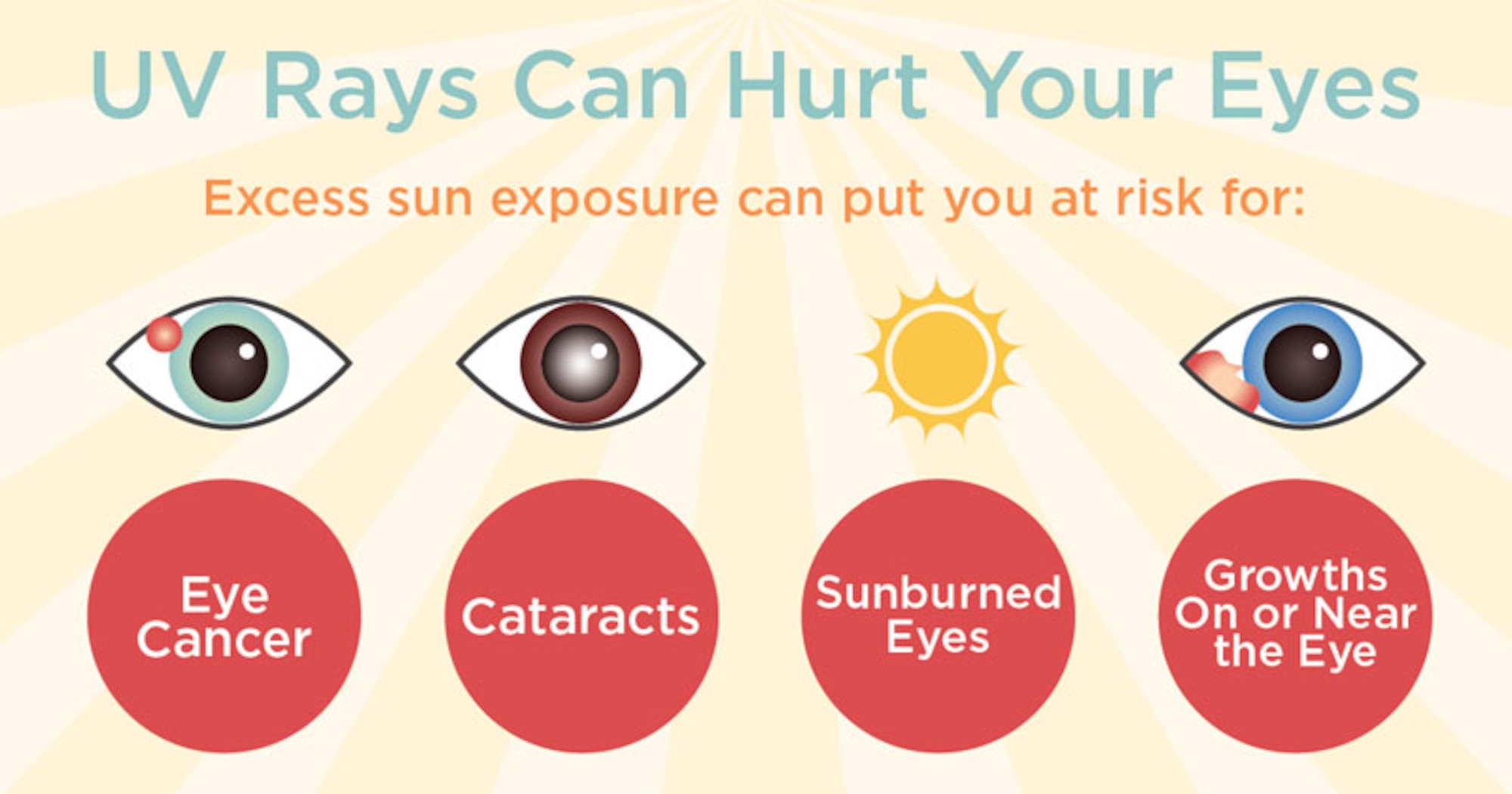





 Prescribing reading glasses effectively treats many of these problems. A convex plus lens relaxes the child’s focusing system, relieving much of the visual stress. In fact, prescribing a low power plus lens is so effective in keeping children’s visual system comfortable during extended close work at school that they are often called “learning lenses.”
Prescribing reading glasses effectively treats many of these problems. A convex plus lens relaxes the child’s focusing system, relieving much of the visual stress. In fact, prescribing a low power plus lens is so effective in keeping children’s visual system comfortable during extended close work at school that they are often called “learning lenses.”
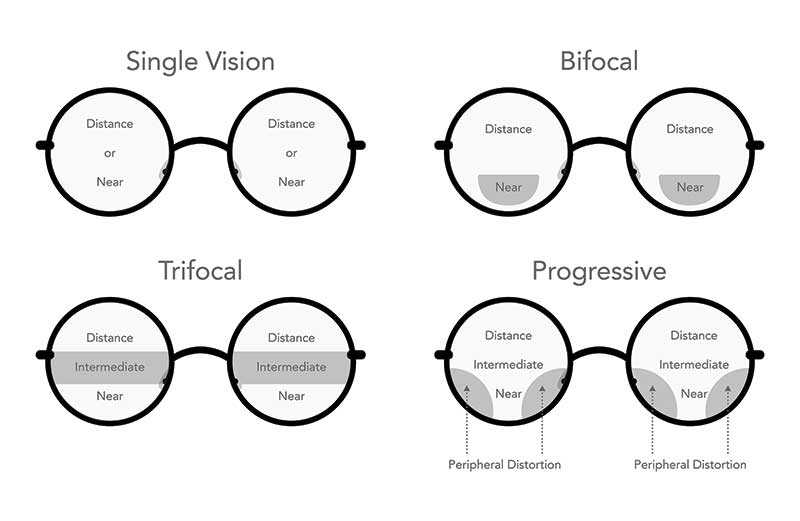





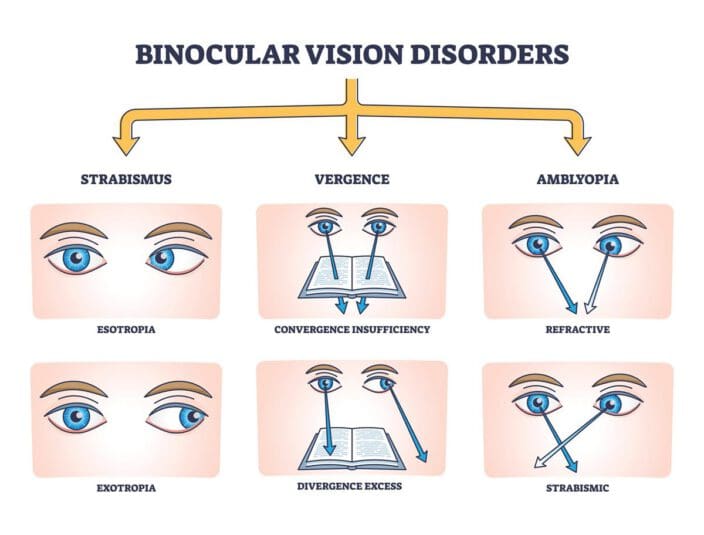









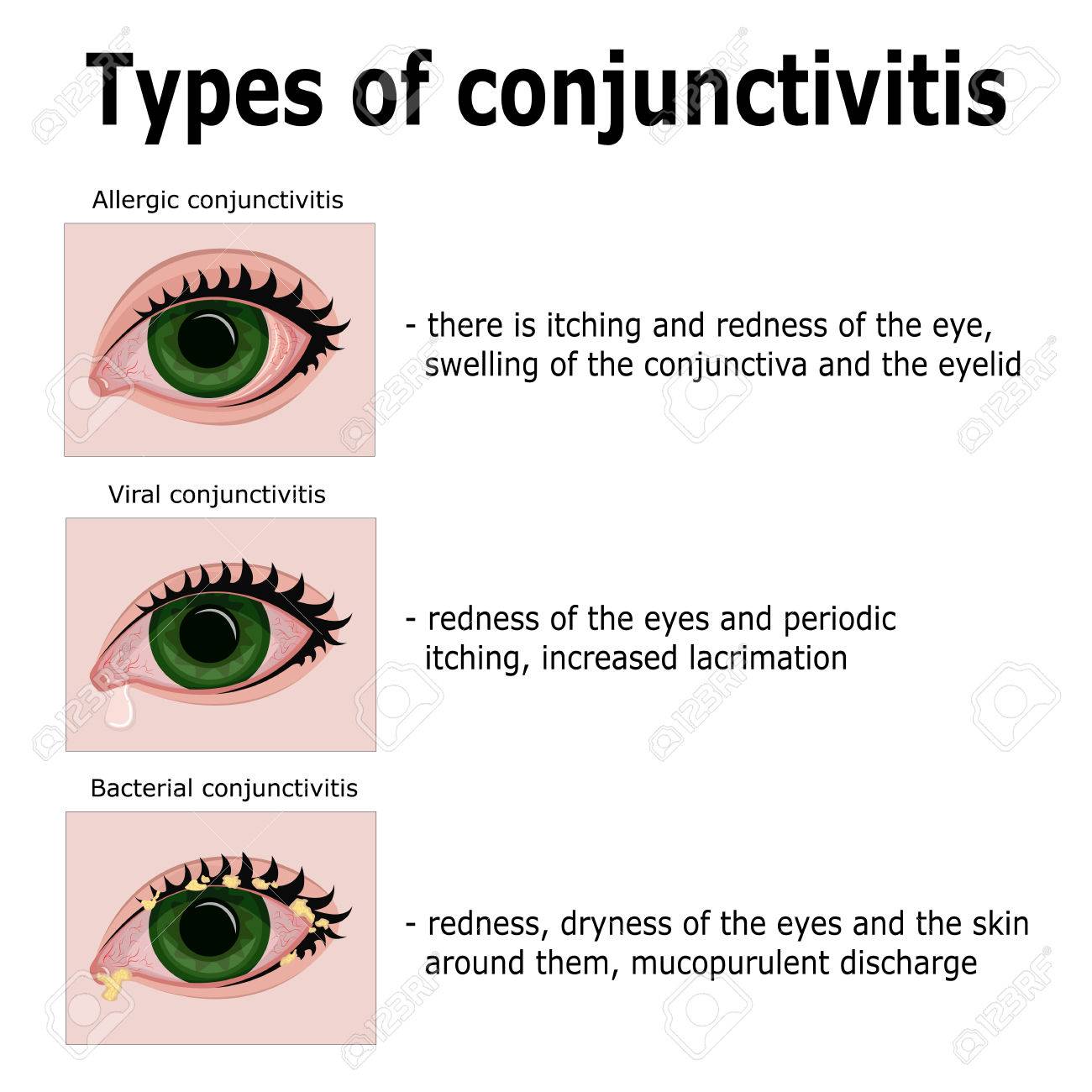










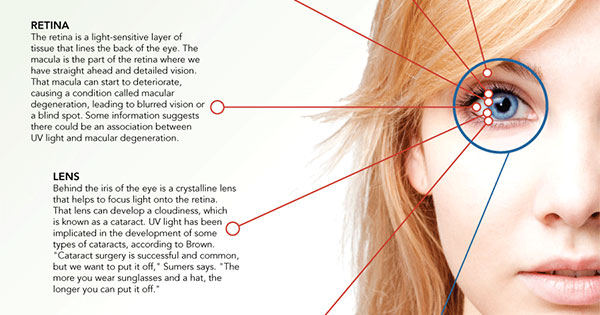





















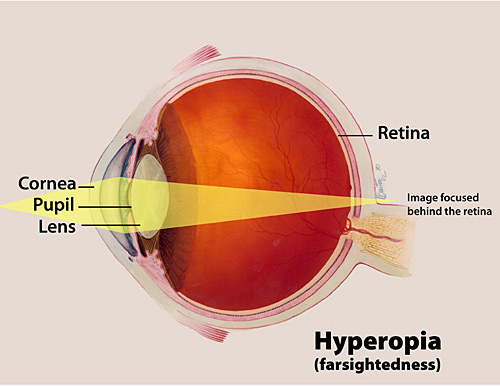


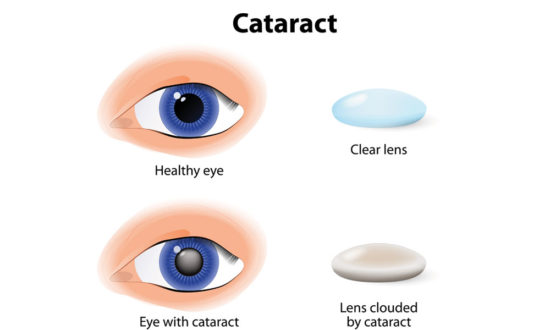








































 وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.
وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.