The definition of a sedentary lifestyle (sometimes called "sitting disease") is one in which a person has no regular physical activity. A typical sedentary person of working age may have a sedentary occupation that keeps him or her seated and using a computer all day. Commuting to and from work in cars or on buses or trains leads to additional time sitting or being still.
For sedentary workers, nights and weekends may involve sporadic or minimal exercise, but for the most part, someone who is sedentary is more likely to be found sitting or lying down in his or her free time too, engaged in one of the following activities:
eating or drinking (socially or alone)
watching TV, sports, or films
reading
sleeping or napping
engaging in non-athletic hobbies (knitting, doing puzzles)
Sedentary behavior and physical inactivity are not only linked to DED, but also to more severe eye conditions, including diabetic retinopathy, AMD, age-related cataract, and glaucoma.
Many people associate a sedentary lifestyle with potential physical health issues. However, it can also affect your cognitive abilities and your mental health.
A sedentary lifestyle can lead to:
Anxiety
ADHD
Obesity
Dementia
Memory issues
Osteoporosis
Chronic Back Pain
Cardiovascular Diseases
Type 2 Diabetes
Depression
Stress
Difficulty concentrating
Physical activity is an effective stress relief strategy and can promote increased energy levels, improved mood, and quality sleep. All of those can play a positive role in supporting your overall well-being. eResearch by Navid Ajamin -- winter 2025
Osteoporosis is a bone disease that develops when bone mineral density and bone mass decreases, or when the quality or structure of bone changes. This can lead to a decrease in bone strength that can increase the risk of broken bones (fractures). Pregnancy, Breastfeeding, and Bone Health.
Dementia is a general term that represents a group of diseases and illnesses that affect your thinking, memory, reasoning, personality, mood and behavior. The decline in mental function interferes with your daily life and activities. It's estimated that about 50% of people age 85 and older have dementia.
? How to reduce sedentary behaviour
Sedentary behavior is any waking behavior characterized by an energy expenditure ≤1.5 metabolic equivalents (METs), while in a sitting, reclining or lying posture. In general this means that any time a person is sitting or lying down, they are engaging in sedentary behaviour.
Most health professionals define a sedentary lifestyle as one that does not meet the Center for Disease Control’s recommendations for exercise. The CDC states that someone should engage in at least 150 minutes of moderate exercise or at least 75 minutes of vigorous physical activity every week. This includes sitting for extended periods and not moving around enough whether during work hours or leisure time.
Lack of exercise is a common cause of a broad range of medical problems that can impact both your physical and mental well-being. Understanding the risks can motivate you to incorporate more physical activity into your daily life, starting with small changes and gradually building up your exercise routine.
When you have cloudy eyesight, it may seem like you're looking at the world through a foggy window.
Cataracts are the most common cause of clouded vision. Most cataracts develop slowly, but usually become worse over time. Cataract surgery is the most effective treatment to help restore your vision.
Cloudy vision, or hazy vision, also means that you can’t see things clearly. However, it doesn’t happen because things are out of focus. Seeing things like you’re looking through a fog, haze or cloud is similar to blurred vision and may even have some of the same causes.
Stress and anxiety can impair many aspects of your health, including your vision. You may experience vision loss or other vision symptoms, like blurriness, light sensitivity, or loss of visual acuity. Chronic stress may speed up the development of eye diseases like macular degeneration or glaucoma.
Medical conditions that can cause Blurred and Foggy vision include:
- diabetes or low blood sugar levels.
- migraine, head injury or concussion.
- pre-eclampsia (high blood pressure) if you are pregnant.
- psoriasis (a skin condition that sometimes can also affect the eyes)
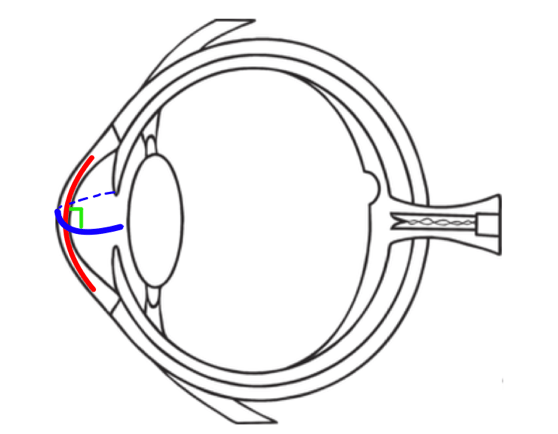
Glasses and contact lens prescriptions with regular astigmatism have two different power numbers, one for each curve in order to focus light together instead of in two separate spots. Unfortunately, prescriptions can only be written for regular astigmatism. Irregular astigmatism is when the two different curves are not perpendicular to each other(blue and red lines, Figure below).
Due to this irregularity, contact lenses need to be personalized to match these curves.
The terms irregular and regular astigmatism are used to describe the curvature of the eye, not necessarily the health of the eye. The eye can have either type of astigmatism and still be considered healthy.
What Causes Irregular Astigmatism?
Not all causes of irregular astigmatism are known, but eye care experts have linked it to systemic and ocular diseases and conditions that cause the cornea to warp or thin, injuries from sports or work, and procedures such as LASIK and other types of vision correction surgery.
Causes of Irregular Astigmatism
Keratoconus: This condition thins and weakens the central cornea until the age of 30-40, causing it to bulge outwards. This thinning causes the cornea to go from being rounded and smooth to being pointed, creating a cone-like shape, and making the corneal surface uneven.
Pellucid marginal degeneration (PMD): This condition is very similar to keratoconus, except that it continues throughout life. Specifically, the lower third of the cornea continues to thin and weaken. This creates a protrusion at the bottom, resembling a belly shape.
Keratoglobus: This condition is also similar to keratoconus, except that the cornea thins and weakens in the periphery creating a very rounded bulging ‘globe’ appearance.
Trauma to the eye: A deep cut or tear, stitches, or warpage from a previous contact lens fitting too tight can change the curves on the cornea.Pellucid Marginal Degeneration vs. Keratoconus
Corneal surgery: Corneal transplant/partial corneal tissue replacements and refractive surgeries can lead to complicationsof changing curves on a cornea.
A list of procedures are as follows:
-DALK (Deep anterior lamellar keratoplasty)
-PKP (Penetrating keratoplasty)
-RK (Radial keratotomy)
-PRK (Photorefractive keratectomy)
-LASIK (Laser in-situ keratomileusis)
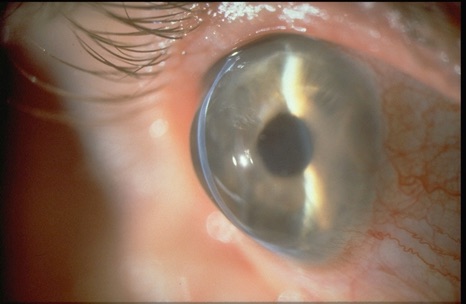
As mentioned above, pellucid marginal degeneration (PMD) is a corneal disease and a rare form of corneal ectasia (a group of disorders that cause the cornea to thin and protrude outward).
Normally, a healthy and thick cornea enables the eyes to see clearly. However, in PMD, the cornea thins over time. This thinning typically occurs in the lower part of the cornea, extending from the 4 o'clock to 8 o'clock position. Above the thinned area, the cornea protrudes outward. These changes in the cornea can lead to astigmatism and a gradual decline in visual acuity.
PMD usually affects both eyes, although it may occur in only one eye in some cases. This condition does not cause scarring in the eyes, allowing the cornea to remain transparent. For reference, the term "pellucid" means clear or transparent.
To date, experts have not yet determined the exact cause or risk factors for developing pellucid marginal degeneration (PMD). However, PMD is more commonly diagnosed when one is in their 20s, 30s, or 40s. While it can also be diagnosed when an individual is in their 50s or older, such cases are rare. So far, there is no scientific evidence suggesting that PMD is hereditary. However, some patients diagnosed with PMD have been recorded to have family members with moderate to severe astigmatism. eResearch by Navid Ajamin -- winter 2025
Treatment
Eye glasses
Most patients can be treated non-surgically with eye glasses, or contact lenses.
Contact lenses
Early stages of PMD may also be managed with soft contact lenses. Success has been shown with the use of rigid contact lenses combined with over-refraction. Patients wearing contacts report increased problems with glare and contrast sensitivity, but it is not clear if this is due to the corneal disease, or the contact lenses themselves.
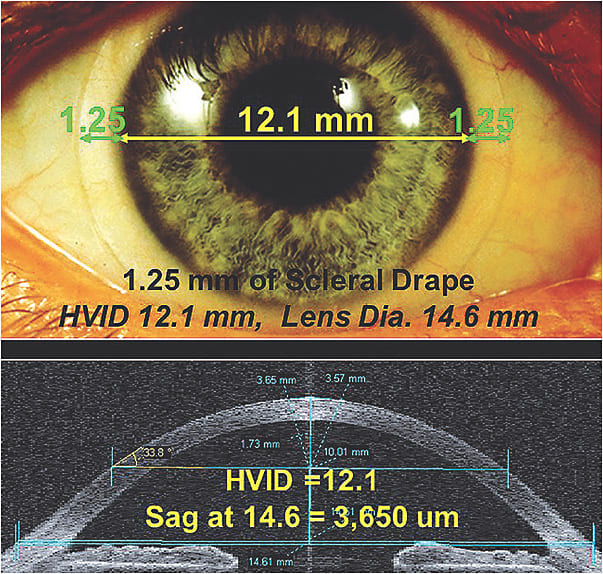
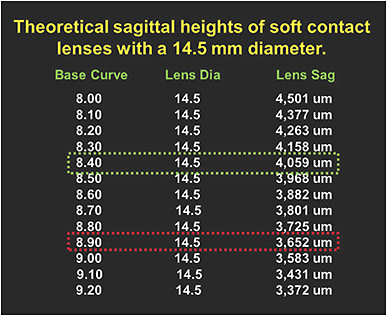
New studies show that the use of a "GP" or Scleral contact lens has shown promise for most patients that exhibit Pellucid Marginal Degeneration. Most of these lenses are in the range of 15.5mm to 18.0mm in diameter.
Regardless of the lens size, it is thought that the larger the GP lens, regardless of the fact that it is a rigid lens, will in most cases be more comfortable then standard rigid corneal lenses, and at times more comfortable than soft lenses.
The highlight to the scleral design and the correction of eye disorders such as Pellucid Marginal Degeneration is that vision with these types of lenses is exceptional when fit correctly.
Intacs
The use of intacs implants has been tested as a treatment for PMD, with slight improvement in visual acuity noted after eleven months,and intacs have been used with keratoconus with success.
Collagen Cross Linking
There is evidence suggesting corneal collagen cross-linking may be beneficial for patients with pellucid marginal degeneration.
Surgery
Corneal transplant surgery may be difficult due to the peripheral thinning of the cornea, even with large and off-center grafts. Therefore, surgery is usually reserved for patients that do not tolerate contact lenses.
Several different surgical approaches may be taken, and no one approach is currently established as the standard.
Examples of surgical procedures used for PMD include: wedge resection, lamellar crescentic resection, penetrating keratoplasty, lamellar keratoplasty, epikeratoplasty and intracorneal segments.
Transplantation of the entire thickness of the cornea (penetrating keratoplasty) may be performed if there is enough normal tissue present. However, if there is not enough normal tissue present, then attaching the graft is difficult.
Due to the thinning of the cornea, PMD patients are poor candidates for procedures such as LASIK and photorefractive keratectomy.
Epidemiology
The incidence and prevalence of PMD are unknown, and no studies have yet investigated its prevalence or incidence. However, it is generally agreed that PMD is a very rare condition. Some uncertainty regarding the incidence of PMD may be attributed to its confusion with keratoconus. PMD is not linked to race or age, although most cases present early in life, between 20 and 40 years of age. While PMD is usually considered to affect men and women equally, some studies suggest that it may affect men more frequently.
Several diseases have been observed in patients with PMD. However, no causal relationships have been established between the any of the associated diseases and the pathogenesis of PMD. Such diseases include: chronic open-angle glaucoma, retinitis pigmentosa, retinal lattice degeneration, scleroderma, kerato-conjunctivitis, eczema, and hyperthyroidism.
Prognosis
Visual function declines as a result of the irregular corneal shape, resulting in astigmatism, and causing a distortion in vision. Deterioration can become severe over time.
SMILE is an acronym for small incision lenticule extraction. While it’s not a perfect acronym of those terms, the “m” is kept from “small” to make it an easier vernacular to use. More importantly, SMILE is a laser eye surgery that uses some of the latest technology. It utilizes a special femtosecond laser to provide incredibly precise sculpting techniques for the surgeon to correct vision issues.
The SMILE procedure involves using the femtosecond laser to build up the matter within the corneal flap. Once the area is shaped, the same laser will make an incision, and the excess tissue will be removed. This effectively creates a new lens shape on the cornea, correcting vision problems. The procedure typically heals within days, and it produces rapid vision improvement.
It’s important to understand that SMILE has been developed specifically to treat nearsightedness. It can be used to treat cataract issues, astigmatism and other sources of nearsightedness.
The Risks and Complications
These are risks, complications, and side-effects. None of these issues are expected to happen. In fact, most of the impact a severe minority of patients, but these issues have been observed and should be considered as possible risks. Here is your complete list of SMILE laser eye surgery side effects.
Night Vision Issues
Any laser surgery has a risk of side-effects regarding night vision. In general, glare from bright lights and halos around lights are known to happen. This doesn’t necessarily afflict patients immediately out of the operation. It can develop years later. The glare and halos can also occur during the day. That said, the issue is usually at its worst when bright lights contrast against general darkness.
ReLEx SMILE _ refractive eye surgery
Night lenses can help deal with the glare and halos, and other treatments may be available for extreme cases.
Debris
The extraction SMILE procedure involves removing tissue from the surface of the cornea. This leads to a possible issue of debris, and it typically stems from the removal of the corneal disc. The debris can include additional problems of its own, including irritation and inflammation.
In extreme cases, the debris may require a followup treatment, but in most cases, it can be flushed with non-invasive treatments. Debris symptoms are typically temporary, but they can add to recovery time and make recovery more complicated in general.
Infection
Any treatment includes a risk of infection. SMILE infection risks are much smaller than most surgical procedures, but the risk does exist. Infections are usually curable when caught early, so it’s important to be on the lookout for symptoms.
Red eyes, excessive itching, pain or a loss of vision are the primary indicators that a patient may be suffering from an infection. Contacting the ophthalmologist immediately is the best way to receive treatment and resolve the issue. Typically, prescription eye drops will be used for a remedy and can even prevent infection in the first place.
Inflammation
While inflammation is not an expectation, it is one of the more common side-effects and is typically accounted for in the recovery process. Inflammation can impact vision and lead to discomfort in the face or headaches.
In the majority of cases, inflammation is temporary and treatable. In extreme cases, it can make recovery more complicated and add to total recovery time. Any pain, vision problems or other signs of inflammation should be communicated to the doctor for treatment.
Clouded Vision
Clouded vision makes everything in sight appear to be hazy. It can be temporary or permanent, depending on circumstances, but it is not a common issue. Clouded vision is at a higher risk for more extreme nearsightedness. Because of this, your doctor should discuss this risk depending on the level of correction you need.
In most cases, clouded vision is not debilitating and is not related to suction loss.
Double Vision
Double vision will most often present as seeing a ghost image. This is a type of double vision called diplopia. It stems from a slight misalignment between the image receptors. When this happens, the brain can struggle to reconcile the separate images coming from each eye. As a result, the ghost image will perform alongside the “true” image.
When severe enough, double vision can lead to follow up procedures for correction. The nature of that followup will be determined case by case, but as the issue is usually created in the surgical process, it is often treatable.
Dry Eyes
This issue is notably less common with SMILE than other laser surgeries. That said, it is still the most common side-effect reported by laser surgery recipients. In most instances, the dry eye symptoms will be at their worst directly after the operation is performed and lessen over time. They can be treated with lubricating drops.
Dryness is a larger concern for people with a pre-existing issue with dryness. The excimer laser can exacerbate those symptoms, and the ophthalmology consultant should discuss this issue beforehand, especially in a case of suction loss.
Miscorrection
It is possible to over or under correct vision problems with a SMILE Lasik operation. This issue is not unique to SMILE. Regardless, vision problems can be worse after the operation than before. In the case of under-correction, vision problems will be reduced, but not to the point of expectation. In overcorrection, nearsightedness may be replaced by farsightedness.
Miscorrection can lead to retreatment. The nature of that treatment will have to be discussed by the surgeon and patient. In some cases, a repeat of a procedure is sufficient. In other cases, a separate procedure may be warranted.
Cornea Bulging
This is one of the most uncommon side-effects of the procedure. It can happen if the eye becomes weak. In that case, the lens will bulge forward. Bulging is an issue that can affect people without ever having refractive surgery. Corrective surgeries increase the risk of bulging in a case of weakened eyes, but it is very uncommon.
Bulging can lead to vision problems. They will typically be treated with corrective glasses or contact lenses. In the most extreme cases, a transplant can be used to resolve the issue.
Blindness
Incision lenticular extraction SMILE involves cutting flesh. That means that the worst-case scenario includes blindness or partial loss of sight. It is exceedingly uncommon, but the risk does exist and must be discussed. Any eye operation can potentially go wrong and lead to blindness. It is something your surgeon should discuss before committing to the procedure.
Other general medical issues can be attached to this treatment course, but they are no more likely with SMILE than any other application. The full list of risks and issues should always be discussed with your doctor before proceeding with treatment.
High Order Aberrations (HOA): It is no surprise that the human eye is not a perfect optical system but suffers from many high order aberrations that degrade the retinal image quality. Light aberration causes blurred vision.
Aberration simply means anything that prevents light from traveling in a straight line. In other words, an aberration causes the ray of light to be misdirected from its desired image point.
Zernike Polynomials are derived by mathematically converting the wavefront error created by a specific aberration and transforming it into a three-dimensional model that mimics the shape of the aberration.
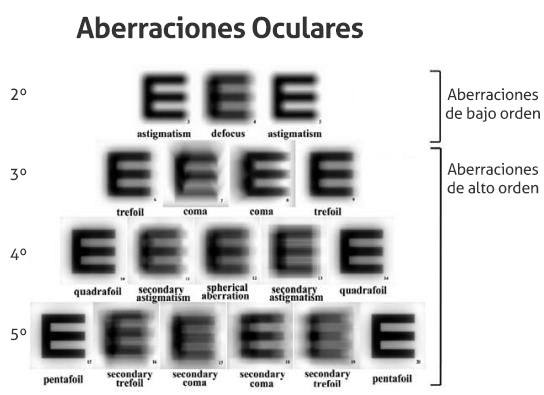
Even though over 65 total aberrations up to the eighth order have been identified, the human eye is able to perceive distortion effects only up to the fifth or sixth order.
Clinically significant High Order Aberrations (HOA) can degrade vision in spite of full correction being used for defocus (Myopia, Hyperopia) and Astigmatism.
There are two main types of light aberrations:
Low Order Aberrations: These aberrations are corrected with prisms, glasses and contact lenses.First-Order Aberrations: These include: Piston (or plano; i.e., no prescription lenses) and Prism correction, which is used if your eyes are misaligned; for example, if you have Crossed Eyes. Prisms divert light from its original path so that you do not have Double Vision.
Second-Order Aberrations: These include: lenses to correct for Myopia, Hyperopia, Presbyopia, and Astigmatism.
High Order Aberrations (HOA): Everything higher than Low Order Aberrations is considered HOA. Your set of HOA is unique to your eye, as your fingerprint is unique to you.
Another way to demonstrate how your vision may be distorted by aberrations is using a tool known as a Point Spread Function (PSF), which uses another mathematical calculation.
Basically, when a point of light passes through the eye, the aberration(s) that eye possesses will disperse or spread the beam, causing the point to blur. The point of light will take on a characteristic appearance when it hits the retina, depending on the aberration(s) present.
What causes HOA?
Any condition that affects the optics of the eye will result in changes in HOA.
These include, but are not limited to:
Tear film abnormalities; for example, as seen in Dry Eyes
Distortion of the cornea as seen in Keratoconus , Pterygium, Corneal Degenerations, Corneal Dystrophies, Corneal Scarring, Corneal Infection or Inflammation, Refractive Surgery, Distortion of the Crystalline Lens as seen in Cataracts and Lens Implants
Even conditions that result in irregular Retina surfaces may create High Order Aberrations such as:
Macular Edema
Epiretinal Membranes
Macular Degeneration
Trauma or Diseases affecting any of the optical components of the eye
Large or slowly-responding pupils because the effects of HOA increase with pupil size.
Pupil issues may be seen in:
Children
Individuals who work in low-light situations
Individuals who take medications that dilate the pupils such as Antidepressants, Beta-blockers, Antihistamines, Amphetamines, and Nitroglycerine
What are symptoms of HOA?
Uncorrected HOA may cause specific bothersome symptoms in vision such as:
Double images
Lack of contrast or crispness
Reduced color perception
Glare sensitivity
Night vision problems
Starburst patterns and/or comet’s tails around lights at night. These complaints may be seen in Third-Order Aberrations such as Coma.
Halos: This complaint may be seen with Fourth-Order Aberrations such as Spherical Aberration.
Decreased distance and near vision: This complaint may be seen with Fourth-Order Aberrations such as Secondary Astigmatism, which can have a negative effect on vision, often described as “central island”-type distortion. The light appears pushed out to the edges of the image.
How are HOA measured?
High Order Aberrations are measured using an aberrometer. There are several commercial brands available which work on the same general concept.
In a nutshell, two or more parallel beams of light are passed through the eye and then a method is used to measure the extent to which those beams cease to travel in a visually optimal path. Complex mathematical formulas then predict aberrations based on the altered angle of those beams.
The most commonly used method today is known as the Shack-Hartmann Method, which is used in several wavefront refractive surgery platforms. In this technique, a bright beam of light is projected into the retina and reflects back out through the eye.
The exiting beam then passes through an array of lenses (called lenslets) where it is split into many tiny beams that project spots of light on a digital camera. The displacement of these spots corresponds to the amount of aberration.
The commercial brands available can give the eye care provider much more information about each patient than he or she ever had previously.
For example, there is a brand of wavefront aberrometer that incorporates auto refraction (estimating the prescription of the patient; i.e. calculating the low-order aberrations), corneal topography (showing a map of the corneal surface), keratometry (measuring corneal curvatures), pupillometry (measuring the distance between the pupils), along with measuring High Order Aberrations.
Corneal abberations can cause vision distortion particularly around bright lights.
(A) Normal vision, (B) halo effect, (C) starburst, and (D) coma.
Provided courtesy of Dr. John Males.
How can HOA be corrected?
HOA can be corrected with spectacle glasses, for example. Some contact lenses companies are touting that their lenses help correct High Oder Aberrations.
In the area of spectacle correction, there is a commercial brand aberrometer available which is a high resolution system measuring more than 11,300 points within a 6 mm pupil diameter.
Benefits of using this equipment include:
You can have your eyeglass prescription calculated in a completely objective way (not relying on your responses of which image is clearer)
Your eye doctor can show you a printout that explains to you your eye’s aberrations.
The process takes only a few minutes for a full measurement
Can provide information to manufacture spectacle lenses to correct many HOA
Because your HOA are as unique to you as your fingerprint, this evaluation is often referred to as an “optical fingerprint,” or “iPrint.”
Not everyone needs to have their HOA corrected and this instrument estimates which patients are most suitable for this correction.
D&q = Anterior chamber is deep and quiet (normal, without inflammation)
AC = Anterior Chamber
ON = Optic Nerve | ONH = Optic Nerve Head
RD = Retinal Detachment
PVD = Posterior Vitreous Detachment
DR = Diabetic Retinopathy | NPDR: Nonproliferative DR | PDR: Proliferative DR
CNV = Choroidal Neovascularization
NVI = Neovascularization of the Iris | NVA = Neovascularization of the Angle | NVD = Neovascularization of the optic Disc | NVE = Neovascularization elsewhere (usually peripheral retina)
Oculomotor apraxia (OMA) is the absence or defect of controlled, voluntary, and purposeful eye movement. It was first described in 1952 by the American ophthalmologist David Glendenning Cogan.
Dr. David Cogan in 1960
People with this condition have difficulty moving their eyes horizontally and moving them quickly. The main difficulty is in saccade initiation, but there is also impaired cancellation of the vestibulo-ocular reflex. Patients have to turn their head in order to compensate for the lack of eye movement initiation in order to follow an object or see objects in their peripheral vision, but they often exceed their target. There is controversy regarding whether OMA should be considered an apraxia, since apraxia is the inability to perform a learned or skilled motor action to command, and saccade initiation is neither a learned nor a skilled action.[1]
Causes
OMA is a neurological condition. Although some brain imaging studies of people with OMA reveal a normal brain, some MRI studies have revealed unusual appearance of some brain areas, in particular the corpus callosum, cerebellum, and fourth ventricle. Oculomotor apraxia can be acquired or congenital. Sometimes no cause is found, in which case it is described as idiopathic.
A person may be born with the parts of the brain for eye movement control not working, or may manifest poor eye movement control in childhood. If any part of the brain that controls eye movement becomes damaged, then OMA may develop. One of the potential causes is bifrontal hemorrhages. In this case, OMA is associated with bilateral lesions of the frontal eye fields (FEF), located in the caudal middle frontal gyrus. The FEF control voluntary eye movements, including saccades, smooth pursuit and vergence. OMA can also be associated with bilateral hemorrhages in the parietal eye fields (PEF). The PEF surround the posterior, medial segment of the intraparietal sulcus. They have a role in reflexive saccades, and send information to the FEF. Since the FEF and PEF have complementary roles in voluntary and reflexive production of saccades, respectively, and they get inputs from different areas of the brain, only bilateral lesions to both the FEF and PEF will cause persistent OMA. Patients with either bilateral FEF or bilateral PEF damage (but not both FEF and PEF) have been shown to regain at least some voluntary saccadic initiation some time after their hemorrhages. Other causes of OMA include brain tumors and cardiovascular problems.[1] eResearch by Navid Ajamin -- winter 2025
The source of OMA is in the central nervous system (brain). The process of initiating eye movements is a complicated neural pathway involving many different structures. Imaging of the brain with magnetic resonance imaging (MRI) is commonly performed when evaluating OMA. Findings may be normal or may reveal poor development of regions of the brain, in particular: the corpus callosum, cerebellum, and/or fourth ventricle. OMA can be an isolated condition, genetic, or associated with other syndromes.
Idiopathic congenital OMA is referred to as Cogan-type and is often associated with developmental delay. Risk factors include gestational and perinatal problems.
Cases have been reported in older individuals after lesions in parts of the brain.
Associated conditons. OMA has been described in a wide range of clinical entities, including metabolic and neurodegenerative conditions. A few examples include: ataxia with oculomotor apraxia, ataxia-telangiectasia, vitamin E deficiency, Gaucher’s disease, and Joubert syndrome.[2] unable to initiate eye movements
The patient is unable to initiate eye movements Inability to saccade and pursue freely When you want to look to the right, you turn your head right to compensate. When you want to look to the left, you compensate by turning your head left.
Some patients have defects in only one direction, left or right.
Some patients have problems with both left and right directions.
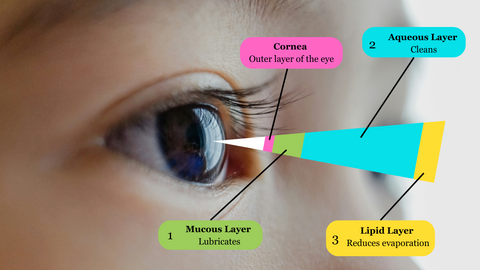
The tear film: The precorneal tear film is approximately 3–5 μm thick [1,2] and is composed of an aqueous-mucin gel phase and an anterior, superficial lipid layer (∼40–100 nm)
The tear film is a protective covering for the cornea composed of three layers:
a surface oily layer
an aqueous layer
deep mucous layer
Previous estimates of tear film thickness suggested that the aqueous layer comprised more than 95% of the tear film, but this has been reduced to 60%, with a larger component being provided by the mucous layer based on evidence from in vivo studies using the confocal corneal microscope.
Effects of tear film dynamics on quality of vision
In addition, clinical evaluation of the tear film involves an assessment of the tear meniscus height (TMH). The TMH reflects the volume of tears that collects at the contact line between the eyelid margin and the bulbar conjunctiva and has several other names, including the inferior marginal strip and the tear prism or rivus.
The ocular surface, tear film, lacrimal glands, and eyelids act as a functional unit to preserve the quality of the refractive surface of the eye and to resist injury and protect the eye against changing bodily and environmental conditions. Events that disturb the homeostasis of this functional unit can result in a vicious cycle of ocular surface disease.
The tear film is the most dynamic structure of the functional unit, and its production and turnover is essential to maintaining the health of the ocular surface. Classically, the tear film is reported to be composed of three layers: the mucin, aqueous, and lipid layers. The boundaries and real thickness of such layers is still under discussion. A dysfunction of any of these layers can result in dry eye disease.
Inadequate tear production can be a result of:
Age (tear production naturally decreases with age)
Preservatives in eye drops (chronic use can impact production and maintenance of the tear film)
Refractive eye surgery like LASIK(can reduce sensitivity to moisture needs, so the eye may not know when to produce more tears)
Some medications
Medical conditions (rheumatoid arthritis, lupus, Grave’s disease, Sjrogren’s syndrome, etc.)
Too much evaporation of the tear film can occur because of:
Dry, windy or smoky environments
Reduced blink rate (such as during prolonged computer use)
Contact lenses (lenses absorb tears)
Meibomian gland dysfunction (decreases the quality/amount of oil produced)
Testing for Dry Eye
Dry eye happens when your eyes don’t make enough tears to stay wet, or when your tears don’t work correctly. This can make your eyes feel uncomfortable, and in some cases it can also cause vision problems.
If your eyes feel dry and scratchy, see your eye doctor. Your eye doctor can do tests to see if your eyes are making enough tears. If the tests show you have dry eye, your doctor can recommend treatment.
Slit lamp test
In a slit lamp test, your eye doctor will use a microscope called a slit lamp to see if your eyes are making enough tears. First, they’ll put a drop in your eye that will make your tears easier to see. Then, they’ll shine a thin, bright light into your eye and look at your eye and eyelids with a microscope.
Schirmer’s test
A Schirmer’s test also tells your eye doctor if your eyes are making enough tears. Your eye doctor will give you eye drops to numb your eye. Then they’ll put a small piece of paper on the edge of your eyelid and ask you to close your eyes for 5 minutes. After 5 minutes, your doctor will see how much moisture (wetness) is on the paper.
Tear break up time (TBUT)
A TBUT test checks how long your tear film (layer of tears on your eyes) lasts after you blink.
Your eye doctor will place a small amount of dye in your eye, and you’ll blink to make the dye fully cover your eye. Then, you’ll look forward without moving your eyes or blinking. Your eye doctor will watch to see how long the dyed tear film covers your whole eye. If your tear film does not last long, you may have dry eye.
Questions:
1. What methods would you use to examine this patient’s tear film quantity?
A. Phenol red thread test
B. Schirmer test
C. Measuring tear meniscus
D. Any of these methods
2. The tear film meniscus height is measured at 0.05mm using the eye-piece graticule. What grade would you record?
A. Low
B. Medium
C. High
3. What factors could be affecting this patient’s tear quantity?
A. Age
B. Environment
C. Medication
D. All these factors
4. Which of the following management options could you consider?
A. Discontinue lens wear
B. Modify lens fit
C. Refit with two-weekly replacement silicone hydrogel lenses that are known to perform well in challenging environments
If you wear contact lenses, you might worry about what happens when they're left outside on extremely hot or cold days. Luckily, a recent study found that as long as the packaging isn't damaged, your contact lenses and their solutions stay safe to use, even in extreme temperatures.
Winter brings icy winds, indoor heating and dry eyes. Contact lenses can still be worn during winter. You may find that wearing contact lenses for dry eyes can boost your comfort. But what about vision quality and eye health in different conditions? Our tips will help you keep vision sharp and eyes feeling healthy, whether you’re working long hours, hitting the ski slopes, or meeting friends for coffee. In winter, your glasses instantly fog up when you come in from the cold. That doesn’t happen with contact lenses.
Tips for wearing contact lenses this winter:
1. Wear sunglasses and contact lenses with UV blocking in the snow, the sun’s rays are strong in winter
2. Keep eyes hydrated - the wind and cold air can cause dry eyes
3. You can wear contact lenses in freezing temperatures
4. If you feel ill, take extra precaution with hand washing before and after handling lenses
For contact lens wearers, there is a high risk of developing dry eyes syndrome due to several factors, such as:
1. Contact lenses can disrupt the natural tear film and interfere with the regular distribution of tears across the eye’s surface. This results in an increased rate of tear evaporation, exacerbating dry eye symptoms.
2. Contact lenses can act as a barrier that limits the oxygen supply to the front surface of the eye. This reduction in oxygen can cause the eyes to become dry and irritated.
3. The materials used in contact lenses can also be a factor in developing dry eyes. Some lenses may have a higher tendency to attract and retain deposits from the tear film or the surrounding environment, leading to increased friction and discomfort.
4. Improper contact lens hygiene or wearing lenses for extended periods without breaks can further contribute to dryness. Failure to clean the lenses properly or using inadequate lens care solutions can result in a buildup of debris and bacteria on the lens surface, which can irritate the eyes and disrupt the tear film.
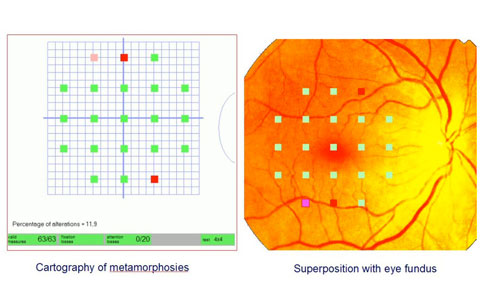
Metamorphopsia is vision dysfunction that causes objects — specifically straight lines — to appear warped, distorted or bent. Rather than a condition itself, metamorphopsia is a symptom. It can result from brain conditions or when there’s a problem with the macula, which is the center of the retina.
somesthetic distortions, including:
Macropsia: Objects appear larger than they are
Micropsia: Objects appear smaller
Teleopsia: Objects seem farther away
Pelopsia: Objects seem closer
Metamorphopsia: Patients perceive their body or body parts as enlarging or shrinking
Chromatopsia: Altered perception of colors
What is metamorphopsia in medical terms?
The term metamorphosis means to change a form or shape of nature into a completely different one. The prefix meta- means after or beyond, the combining form -morph/o means shape and the suffix -sis means an abnormal condition or process.
Metamorphopsia (“meta-more-FOP-see-ya”) is a medical term used to describe an abnormal visual perception in which images appear distorted. For example, straight lines appear curved or jagged. It is an important symptom of retinal disease. Metamorphopsia is not caused by the need for new glasses, cataract, glaucoma, or optic nerve damage. Metamorphopsia is a sign of a retinal problem. It is detected and monitored with an Amsler grid.
The retina is a thin layer of tissue at the back of the eye that uses light to create signals. Signals are sent to the brain through the optic nerve, and registered as an image. The macula is in the middle of the retina and gives us color vision, central vision and visual acuity.
When the retina or macula are affected by age, trauma or disease, metamorphopsia can result. It may affect one or both eyes and may only involve a portion of the vision in the affected eye. Metamorphopsia can potentially indicate the presence of a serious underlying medical cause.
What does metamorphopsia look like?
Metamorphopsia affects central vision. This means objects in your peripheral vision will likely appear normal, while things in front of you are distorted. While metamorphopsia is a symptom in itself, some signs to look out for include:
Objects that are normally straight appear curved or warped. Example: A light pole looking bent or “melted.”
Things that are normally flat appear rounded. Example: A frisbee looking like a bowl.
Borders on objects appear smudged or distorted. Example: The face of a watch looks like someone smeared the edges of it.
Objects change shape. Example: A rectangular door frame twists out of shape.
Things look disproportionately larger than normal (macropsia).
Things look disproportionately smaller than normal (micropsia).
If you experience any of the symptoms listed above without explanation, seek help from an eye doctor or medical professional.
How is metamorphopsia diagnosed?
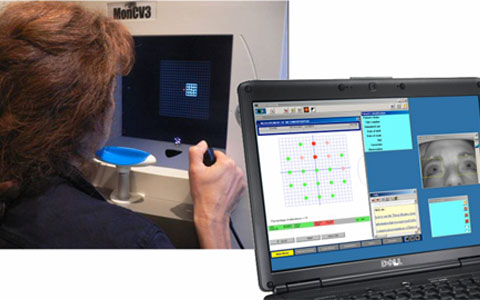
Your eye doctor may run a series of tests to determine whether you have metamorphopsia and how severe it is. The tests usually involve having the patient look at some type of chart and answering questions about what they see. Some tests used to measure metamorphopsia include:
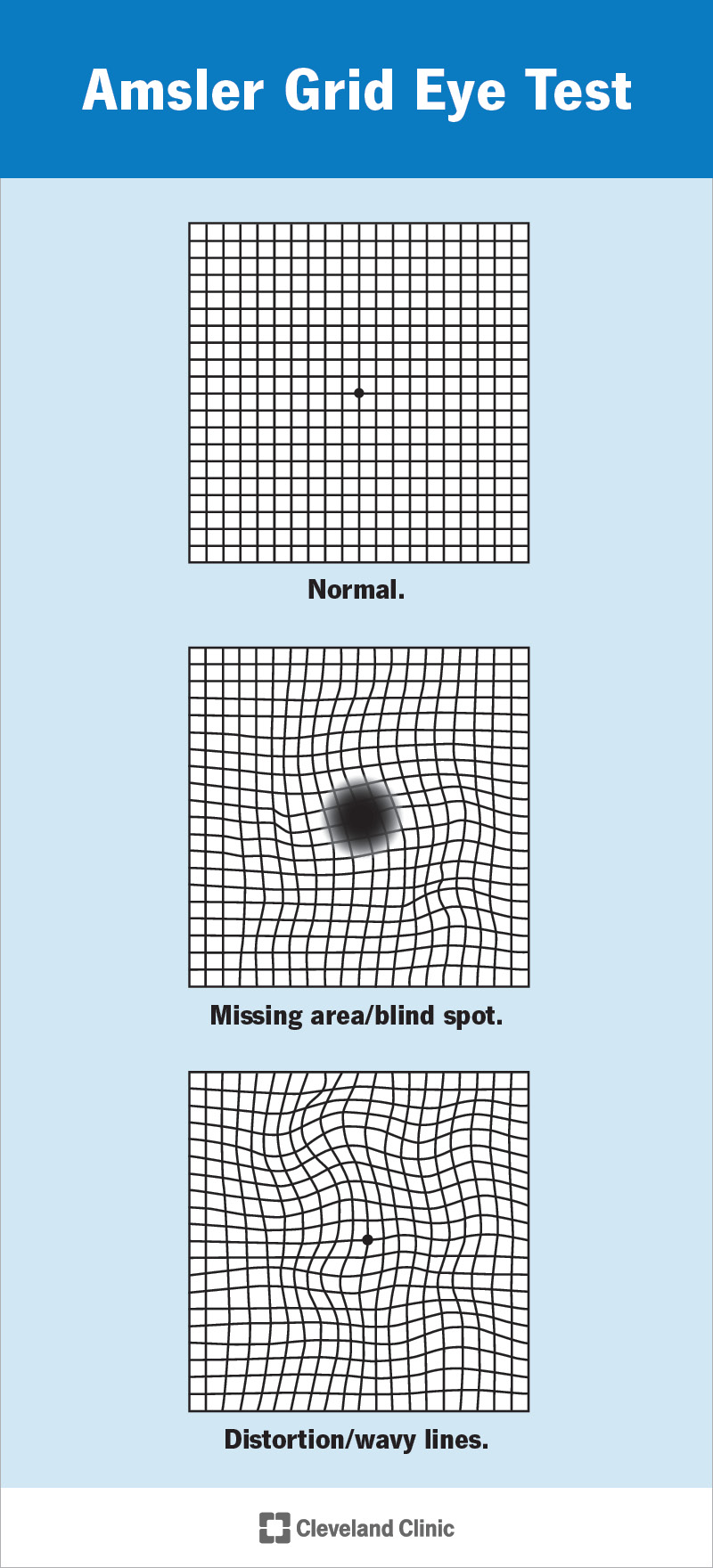
Amsler grid
Amsler grid for metamorphopsia is the most well-known and the most commonly used test that doctors use. It involves looking at a box with equally spaced horizontal and vertical lines that create a grid. In the middle of the grid is a small dot.
To take the test, the patient must be wearing corrective lenses, reading glasses or whatever is required for them to have their best corrected vision. Then, they focus on the dot in the middle of the grid while covering one eye at a time. This part is especially important, as looking at the grid with both eyes can cause the good eye to compensate for the bad eye.
While focusing on the dot in the middle, the patient should pay attention to how the lines around the dot appear. If they still appear straight, metamorphopsia isn’t the problem. If these lines appear curved or warped, metamorphopsia may be the problem.
A patient’s perspective of metamorphopsia (B) compared to normal (A)
M-chart
The M-chart is more specific than the Amsler grid, but it isn’t used as often. It was created to help pinpoint the degree of metamorphopsia and whether the distortion is more present in horizontal or vertical lines.
The test has 19 dotted lines, starting with a straight line (zero degrees). The size and space between the dots that create the line gradually go from very fine (0.2 degrees) to coarse (2.0 degrees). Each line has a dot in the middle of it that the patient is supposed to focus on.
Starting with the straight, solid line, the patient will focus on the dot and tell the doctor whether the line looks curved in places or not. They do this for every line, from fine to coarse, until the line no longer looks distorted to the patient.
Once this is recorded, the doctor will turn the M-chart 90 degrees (making vertical lines horizontal or vice versa). The patient will perform the test again. eResearch by Navid Ajamin -- winter 2025
The farther the patient goes before the line no longer looks curved, the more severe their metamorphopsia is. It’s also recorded whether vertical or horizontal lines are affected more than the other.
Possible Causes
What are the most common causes of metamorphopsias?
Depending on why they happen, metamorphopsias can be a minor annoyance or a sign of serious problems. There are three main sources of metamorphopsias:
Refraction conditions and changes (most common).
Retinal changes and conditions.
Brain-related conditions (least common).
Refraction conditions and changes
Your eye bends (refracts) light as it enters and passes through. That bending is supposed to focus light beams precisely on your retina. The more precise the focus, the clearer you see. Refractive errors are when that refracting doesn’t happen correctly. Examples include:
Strong or severe refractive errors like astigmatism.
A large difference in prescription strength needs between your eyes (anisometropia).
Cornea or lens shape changes/differences.
New corrective lenses (like eyeglasses or contacts), especially with bigger changes to how you see.
What Is the Amsler Grid
Retinal changes and conditions
The retina at the back of your eye has a light-detecting layer of cells (photoreceptors). Part of how they work is due to the shape of your retina, which needs to lay flat against the layer underneath.
Wrinkles, holes or other retinal changes can cause metamorphopsias when they change the shape or position of your retina. Metamorphopsias are more severe when they happen in the macula, the part of your retina responsible for detecting color and fine details.
Your retina needs light to arrive with precise timing, so changes in your retina’s shape distort what you see if the light arrives too early. And if the changes in your retinal shape or position are severe, it can destroy the connections that let your retinas send light-related signals to your brain. When that happens, it can cause permanent vision loss or even blindness.
Retinal and retina-related conditions that can cause metamorphopsias include:
Age-related macular degeneration, especially the wet form.
Central serous retinopathy.
Chorioretinopathy conditions like chorioretinitis.
Cystoid macular edema.
Diabetes-related retinopathy and diabetes-related macular edema (swelling).
Macular pucker.
Ocular migraine.
Retinal bleeding (hemorrhage).
Retinal tears or detachments.
Retinitis pigmentosa.
Uveitis, including choroid inflammation from infection-related conditions like presumed ocular histoplasmosis syndrome.
When you're sleep deprived, your eyes don't have a chance to rest and recover from the day's activities. This can lead to several vision problems, including: Blurry vision.
How lack of sleep affects your eyesight ?
It can be easy to spot someone who did not get enough sleep: dark circles, puffy eyes, or drooping eyelids can be signs of a poor night’s rest.
However, a lack of sleep affects more than just your appearance. Sleep is fundamental to your health and well-being. Skimping on your beauty rest affects your mood, motivation, memory, metabolism, and so much more. It even affects the health of your eyes.
Sleep deprivation and eye health
Much like the brain and the body, your eyes heal themselves as you sleep. Not getting enough sleep can lead to having dry, itchy, or bloodshot eyes. The eyes may produce less tears after a night of insufficient sleep. This can open the door to eye infections.
You may experience eye twitches or spasms when you have not had enough sleep. Your eyes may even be more sensitive to light, or you may have blurry vision. Sleep deprivation could lead to serious eye problems, such as glaucoma, over time.
Sleep apnea and your eyes
What does sleep apnea have to do with your eyes?
Sleep apnea is a risk factor for glaucoma. Glaucoma is an eye disease that could lead to loss of vision. The likelihood of developing glaucoma is higher in people who have sleep apnea.
Eye doctors may be able to spot signs of sleep apnea during a routine eye exam. Changes in your eyelids, retina, or vision could be indicators of sleep apnea. When sleep apnea is treated, many of the eye-related symptoms are reversible.
Tonight, give your eyes a chance to rest and heal by getting your recommended amount of sleep. Adults should sleep seven or more hours per night on a regular basis. To support your overall health and the health of your eyes, follow these healthy sleep tips.
Prescription eyeglasses have become a major demand by majority of the people these days worldwide, as the usage of digital devices such as computers, LED TV’s and mobile phones, etc. are being vastly used by individuals of every age as well as children. But fortunately, there is an arrival of a latest and a revolutionary technology that can highly assist those, who love to see the world clearly than ever before.
This latest technology in eyeglass industry is known as Free-Form Progressive Lenses," a groundbreaking digital manufacturing procedure, making use of computer-assisted design and developing to produce a futuristic, customized eyeglass lenses according to your provided prescription.
Just imagine that you go for shopping to get a new pair of pants from a branded store, and that is slightly longer or unfitted on you. So what would you ask them? Certainly to get it customized, so it fits perfectly and making you look exceptional. The same thing happened here as you can now get your current lenses customized for particular prescriptions and frames.
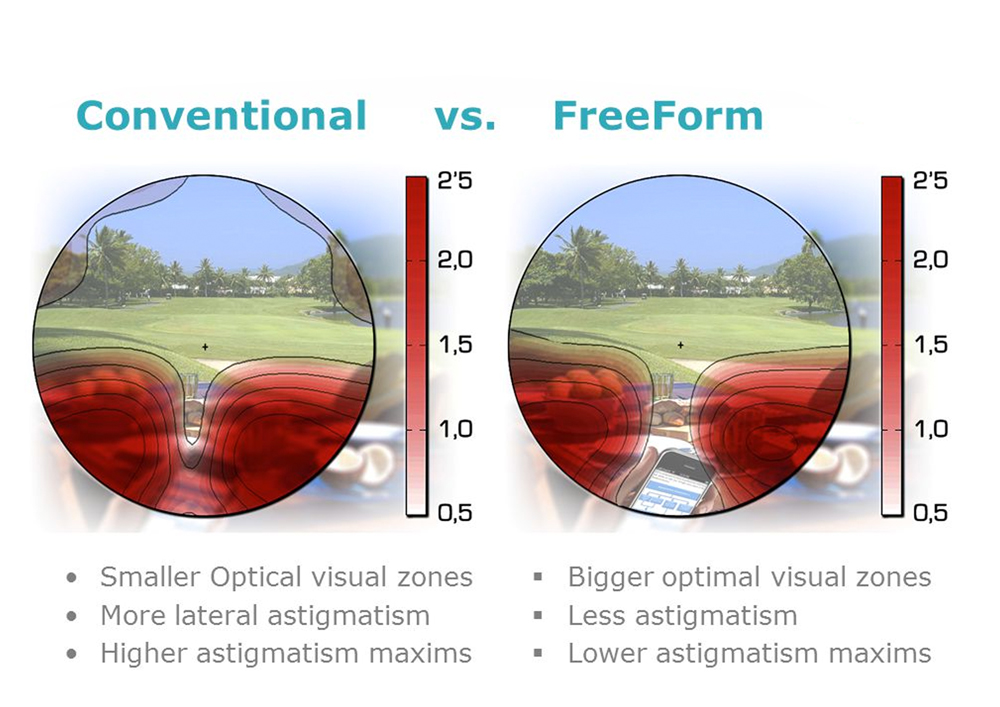
Difference Between Standard & Free Form Lenses
Free form lenses are among the prevalent types of advanced lenses, produced by utilizing free form technology, letting users to attain improved optics. Let’s discuss the main comparison of standard & free form lenses:
Standard Lenses:
Standard lenses are mainly the pre-molded lens, having the progressive design formed on its front exterior. In its production, the prescription is created on its back surface and this way the mold is not changed.
These are digitally designed that is made via software measuring a person’s prescription and some additional factors like frame fitting position. What is does is it lets them to be modified according to every person rather than simply using pre-molded lenses. If you can recall the very first time you came to see any high-definition LED TV, could you imagine how you compared it with the analog TV picture? It definitely would have appears crispier as well as clear, didn’t it! Now think similarly this matter with your prescription glasses and you will perhaps see more satisfactorily with the lenses you are using, but wouldn’t it be beneficial if you could do advancement to high-definition for your eyes?
Advantages of using Free-form Progressive Lenses Some top-ranking eyeglasses companies such as Goggles4u believes that the free-form progressive lenses technology could be the revolution in vision improvement. Furthermore, it can also recover eyesight precision that custom-made free form lenses deliver. With this type of lenses, you can expect to achieve:
Excellent Low-Light & Night Vision: These free-form lenses have the ability to decrease the glare and radiance effects produced by light causes in the dark, such as those from a car’s headlights.
Reference:
reddoptical.co.zw/what-we-do
2020mag.com/ce/the-optics-of-free-form
Advantages of Free Form Progressive Lenses (goodrichoptical.com)
Notes that after viewing at near distances for several hours, observers may become temporarily myopic. This effect, known as transient myopiaafter visual work, was studied by measuring contrast sensitivity to a sinusoidally modulated grating pattern.
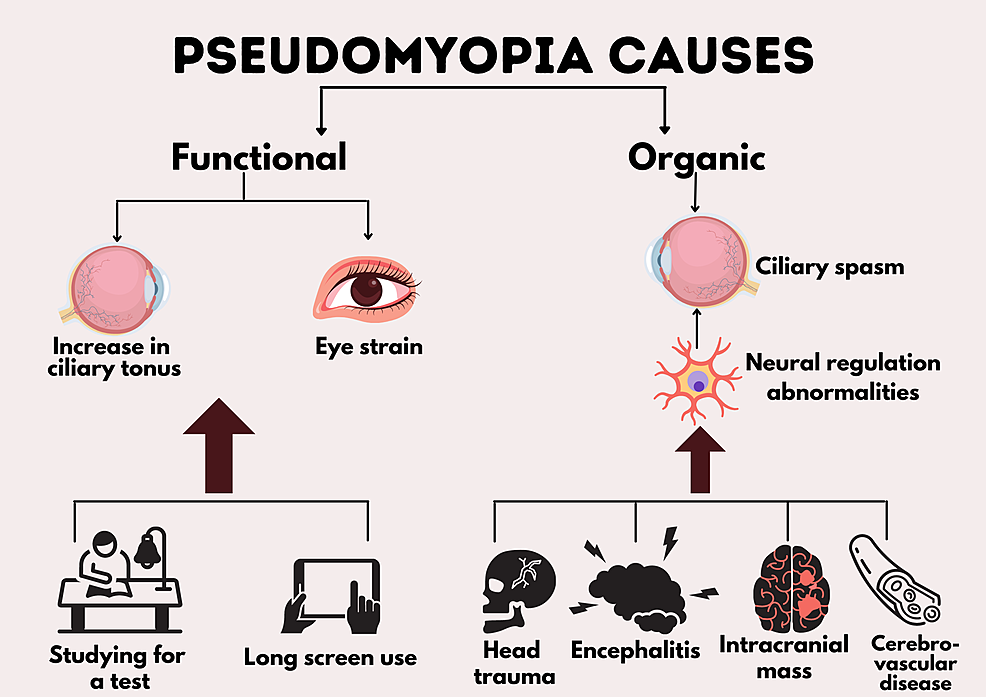
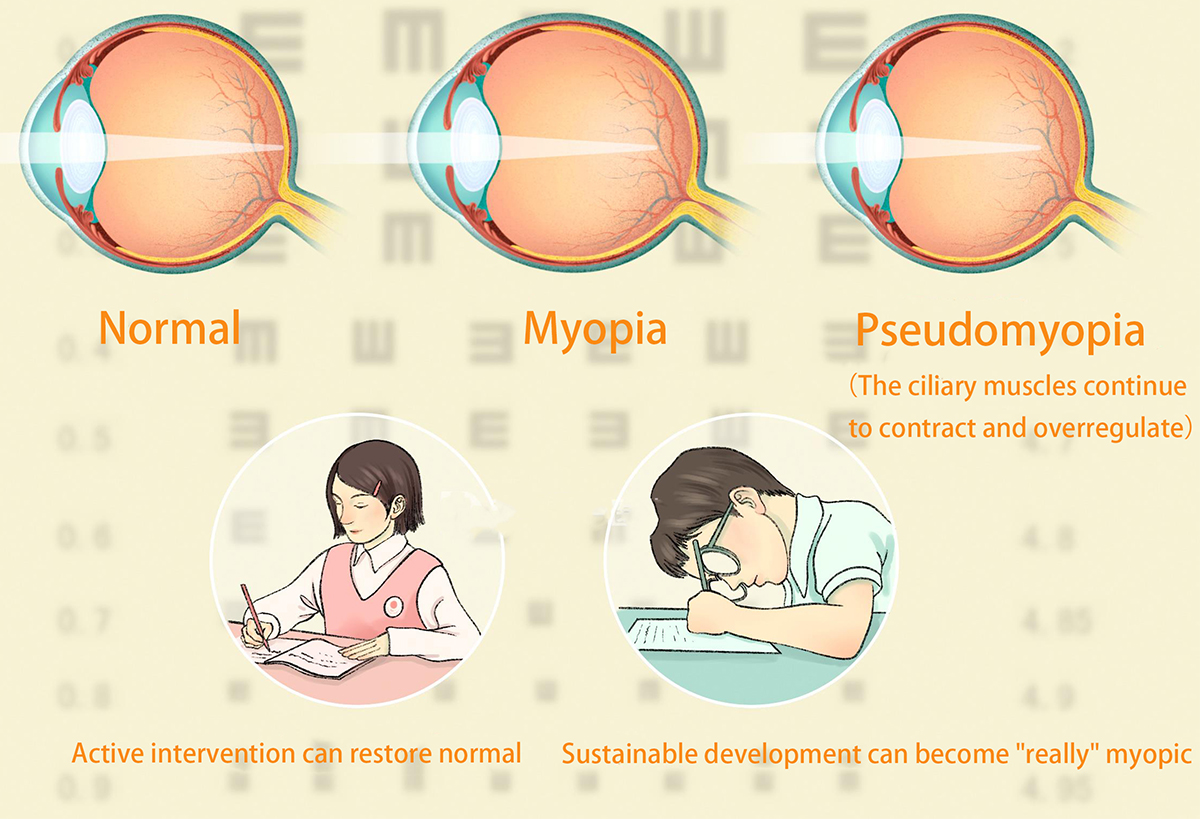
Prolonged activities such as reading, writing, using computers, tablets, and smartphones without resting the eyes can cause the eye muscles to remain contracted, leading to blurred distance vision. This condition is what we refer to as pseudomyopia.
Pseudomyopia(from ψεῦδο, "pseudo": false; and μυωπία "myopia": near sight
Pseudomyopia is an inappropriately excessive accommodation of the eye due to overstimulation or ciliary spasm, which leads to a marked approximation of the far point.
Most people do not understand "pseudomyopia". Pseudomyopia is generally easy to appear in childhood, and parents simply think that pseudomyopia does not need to be dealt with, and the child's vision will automatically recover after a period of rest. Most parents still take a fluke and think that their children are still young, which must be pseudo-myopia, and there is no need to specifically check them, but in fact, this practice actually delays the children.
"Pseudo-myopia" does not belong to the true sense of myopia. It is actually a type of ciliary muscle that is continuously contracted and spasm due to excessive adjustment, and the thickness of the lens increases, so that the image of the object is in front of the retina, because its symptoms are the same as myopia. But it is essentially different from myopia, so it is called "pseudo-myopia".
Pseudo-myopia is a functional abnormality and is reversible!
transient myopia and esotropia
Transient myopia, which can also be called accommodative spasm or pseudomyopia, occurs when the accommodative system is not relaxed, making a patient falsely seem to need more minus lens correction power.
Nearwork-inducedtransient myopia (NITM), a lenticular-based pseudomyopia, is commonly found in myopic teenagers and young adults. It has been speculated that its presence may be a factor in nearwork-related symptoms and in the development of permanent myopia.
What is anxiety?
Feeling anxious is a normal part of life.
Many people worry about things such as health, money, school, work, or family. But anxiety disorders involve more than occasional worry or fear. For people with these disorders, anxiety does not go away, is felt in many situations, and can get worse over time.
Common symptoms of pseudomyopia include eye strain or fatigue, and it is classified as organic or functional.
The latter is due to eye strain and functional increase in the ciliary tonus. Pseudomyopia can vary from being a transient condition or continue to progress to myopia. Head trauma is the most common cause followed by psychiatric illnesses, neurologic diseases, and drug-induced causes. There is an association between psychological stress-inducing events and pseudomyopia as it affects the autonomic nervous system. The human body counteracts anxiety by activating the parasympathetic nervous system, causing ciliary muscle contraction.
What is the cause of pseudomyopia?
Pseudomyopia or accommodative spasm occurs because of excessive constriction of theciliary muscle which clinically manifests as blurred vision, distorted image, photophobia, and ocular pain. Symptoms are variable and can be unilateral or bilateral and constant or episodic
What is the difference between myopia and pseudo myopia?
Myopia is a major health problem leading to significant public health and economic concerns, especially in Asia.
Pseudomyopia refers to spherical equivalent (SE) ≤−0.50 diopters (D) before cycloplegia and >−0.50D after cycloplegia, and nearly 24.1% of Chinese children were found to have pseudomyopia.
Whether the presence of pseudomyopia affects the risk of myopia remains unknown.
The following symptoms may be seen in patients with pseudomyopia:
+Blurring of distance vision:Intermittent blurring of distant vision after prolonged near work is the main symptom of pseudomyopia.
- Esotropia:Acute onset esotropia may occur in accommodative spasm, which is the common cause of pseudomyopia.
- Diplopia:Diplopia may occur due to esotropia or convergence spasm
+ AsthenopiaEye Strain Can Cause Pseudomyopia
- Headache
+ Eyestrain
- Photophobia
The diagnosis is done by cycloplegic refraction using a strong cycloplegic like atropine or homatropine eye drops. Accommodative amplitude and facility may be reduced as a result of the ciliary muscle spasm.
There is a close correlation between unaided distance visual acuity and myopia; however, this correlation is not maintained in the presence of pseudomyopia, while pseudomyopia maybe presented as decrement of distance visual acuity.
Underlying psychiatric diseases in pseudomyopia patients have been reported in the past in multiple studies. Generalized anxiety disorder is the most common psychiatric illness associated with pseudomyopia with a positive correlation between anxiety-somatization scores and accommodation amount of the eye.
It is strongly advised that a psychiatric consultation should be included in the multidisciplinary evaluation of every case. If patients have coexisting anxiety disorders, a multidisciplinary approach using psychiatric consultations, work environment changes, ocular exercises, and cycloplegic drugs can be used.
This review aims to shed light on the association of psychiatric disorders such as anxiety with pseudomyopia. eResearch by Navid Ajamin -- winter 2025
Do you need glasses for pseudomyopia?
Treatment may include various eye drops or prescription glasses. The duration of treatment for pseudomyopia varies from patient to patient.”
Is pseudomyopia permanent?
In optometry, this shows nearsightedness, but it is not permanent. In most cases pseudomyopia occurs in children between the age of six years old through adolescence. It is less common after that age. In adults, pseudomyopia is rare because the gazing mechanism, so common in children, diminishes as people age.
What is the difference between myopia and degenerative myopia?
Degenerative myopia is typically a consequence of high myopia, a severe degree of nearsightedness. However, degenerative myopia is not merely a degree of myopia but is a distinct form characterized by specific degenerative changes occurring at the back of the eye.
Which drug produces transient myopia?
Drugs known to produce this effect include sulfa drugs and other medications. The possible mechanism is thought to be an allergic reaction to the drug. Both ciliary muscle contraction and ciliary body edema may play role in the pathomechanism.
- Transient Myopia After Acetazolamide
- Transient Myopia Due to Tetracycline
Can pseudomyopia turn into real myopia?
Based on a large prospective population-based cohort study, we found that pseudomyopia was an independent risk factor for myopia development among school-aged children.
Cataract surgery is a procedure to remove the lens of the eye and, in most cases, replace it with an artificial lens. A cataract causes the lens to become cloudy when it is typically clear. Cataracts can eventually affect vision. Cataract surgery is performed by an eye doctor, also called an ophthalmologist.
Cataract surgery replaces the cloudy lens inside the eye with an artificial lens. Cataracts are common as you age, and surgery is usually safe and effective. Depending on your replacement lens, you may need glasses after cataract surgery.
It's normal to have:
grittiness
watering
blurred vision
double vision
a red or bloodshot eye
These side effects usually improve within a few days, but it can take 4 to 6 weeks to recover fully.
For the first few weeks after surgery:
Do:
use your eye drops as instructed
take it easy for the first 2 to 3 days
use your eye shield at night for at least a week
take painkillers if you need to
bathe or shower yourself as usual
wear your eye shield when washing your hair
read, watch TV and use a computer
use your shield, old glasses or sunglasses outdoors
avoid swimming for 4 to 6 weeks
What should you not do after a cataract operation?
Don't:
do not rub your eyes.
do not allow soap or shampoo to get into your eye.
do not drive until you get the all-clear from your doctor.
do not do any strenuous exercise or housework.
do not wear eye make-up for at least 4 weeks.
do not fly without seeking advice from your doctor.
Which glasses are best after cataract surgery?
Polarized lenses – Shop for cataract surgery sunglasses with polarized lenses, which reduce glare and are especially good for driving, says Dr. Khan. “They're going to give you a crisper image, and that comes in handy any time clarity of vision is important,” she says.
Who needs glasses after cataract surgery?
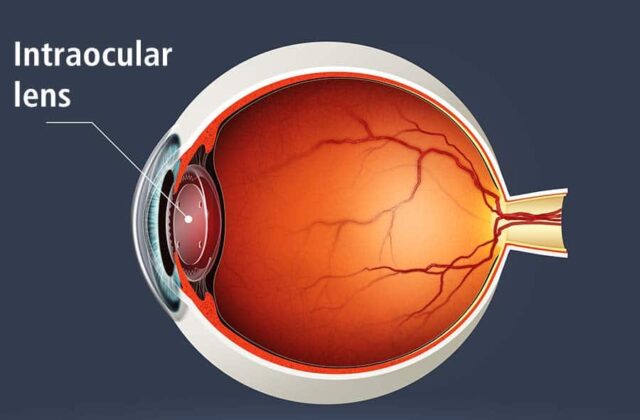
The lens is a curved piece of clear tissue in your eye. Situated behind your pupil, it changes the way light enters your eye and helps you focus your vision at different distances.
Cataract surgery involves replacing the lens in your eye with an artificial replacement called an intraocular lens (IOL). Whether you’ll need glasses after cataract surgery largely depends on what type of IOL you get.
What Is The Best Lens For Your Cataract Surgery
There are many IOL options. Take the time to talk with your eye surgeon beforehand so that you make the choice that’s right for you
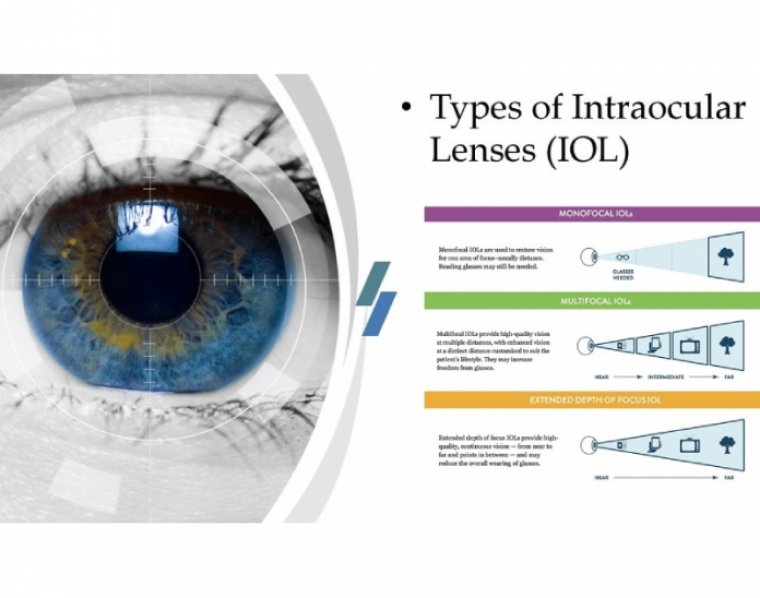
The main types of IOLs include:
Monofocal:Monofocal IOLs are the most common, and also the only IOL that is usually covered by Medicaid and private health insurance. They focus at only one distance, either close, far, or intermediate range. Most people get them for distance vision.
Multifocal:Multifocal IOLs provide both distant and near focus at the same time. They contain different zones, shaped like concentric rings, that allow you to focus on objects far away as well as objects close up.
Extended depth of focus: Extended depth of focus IOLs have only one corrective zone. This zone is stretched to allow distance and intermediate vision.
Accommodative: Accommodative IOLs change shape like your eye’s natural lens to allow you to focus at different distances.
Toric: Toric IOLs correct astigmatism, a vision issue that’s caused by an irregularly shaped cornea.
Light-adjustable lens (LAL):This newer type of IOL is the only one that can be customized after surgery. Adjustments are done through a series of office-based light treatment procedures.
How long should you wait before getting new prescription glasses after cataract surgery?
It’s important to wait for your eyes to fully heal and your vision to stabilize before getting a new prescription. Eye doctors often recommend waiting around 6 weeks after your surgery before having your eyes tested and getting new glasses.
Are there any signs that indicate you need new glasses?
New Glasses After Cataract Surgery
It’s typical to have some blurriness and trouble seeing for a few days after cataract surgery. If you notice persistent changes to your vision, you may need to change your prescription.
Some vision changes you might notice include:
blurry vision
squinting a lot
tired eyes
frequent headaches
light sensitivity
How do you know which glasses are right for you?
After you’ve healed from your cataract surgery, your eye doctor will perform an updated refraction to determine which eyeglass prescription is best for you. It’s most common that people who undergo cataract surgery will need reading glasses after their vision has stabilized.
CME (Cystoid macular edema) is the most frequent complication after an uncomplicated cataract surgery.
What are the negatives of cataract surgery?
Is there a downside to having cataract surgery? While generally safe and effective, cataract surgery carries risks like any surgery, including infection, swelling, and vision issues. However, serious complications are rare.
وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.








.jpg)
/ectasia-visual-simulation-NF(425).jpg)
.jpg)













:max_bytes(150000):strip_icc()/GettyImages-705007087-7358fa86b9ce4600b507e88871ddb5f9.jpg)











 وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.
وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.