The tear film: The precorneal tear film is approximately 3–5 μm thick [1,2] and is composed of an aqueous-mucin gel phase and an anterior, superficial lipid layer (∼40–100 nm)
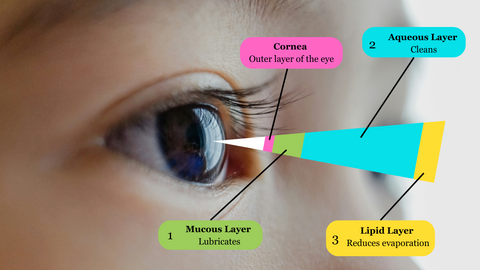
The tear film is a protective covering for the cornea composed of three layers:
- a surface oily layer
- an aqueous layer
- deep mucous layer
Previous estimates of tear film thickness suggested that the aqueous layer comprised more than 95% of the tear film, but this has been reduced to 60%, with a larger component being provided by the mucous layer based on evidence from in vivo studies using the confocal corneal microscope.

In addition, clinical evaluation of the tear film involves an assessment of the tear meniscus height (TMH). The TMH reflects the volume of tears that collects at the contact line between the eyelid margin and the bulbar conjunctiva and has several other names, including the inferior marginal strip and the tear prism or rivus.
The ocular surface, tear film, lacrimal glands, and eyelids act as a functional unit to preserve the quality of the refractive surface of the eye and to resist injury and protect the eye against changing bodily and environmental conditions. Events that disturb the homeostasis of this functional unit can result in a vicious cycle of ocular surface disease.
The tear film is the most dynamic structure of the functional unit, and its production and turnover is essential to maintaining the health of the ocular surface. Classically, the tear film is reported to be composed of three layers: the mucin, aqueous, and lipid layers. The boundaries and real thickness of such layers is still under discussion. A dysfunction of any of these layers can result in dry eye disease.
Inadequate tear production can be a result of:
Age (tear production naturally decreases with age)
Preservatives in eye drops (chronic use can impact production and maintenance of the tear film)
Refractive eye surgery like LASIK (can reduce sensitivity to moisture needs, so the eye may not know when to produce more tears)
Some medications
Medical conditions (rheumatoid arthritis, lupus, Grave’s disease, Sjrogren’s syndrome, etc.)
Too much evaporation of the tear film can occur because of:
Dry, windy or smoky environments
Reduced blink rate (such as during prolonged computer use)
Contact lenses (lenses absorb tears)
Meibomian gland dysfunction (decreases the quality/amount of oil produced)

Testing for Dry Eye
Dry eye happens when your eyes don’t make enough tears to stay wet, or when your tears don’t work correctly. This can make your eyes feel uncomfortable, and in some cases it can also cause vision problems.
If your eyes feel dry and scratchy, see your eye doctor. Your eye doctor can do tests to see if your eyes are making enough tears. If the tests show you have dry eye, your doctor can recommend treatment.
Slit lamp test
In a slit lamp test, your eye doctor will use a microscope called a slit lamp to see if your eyes are making enough tears. First, they’ll put a drop in your eye that will make your tears easier to see. Then, they’ll shine a thin, bright light into your eye and look at your eye and eyelids with a microscope.
Schirmer’s test
A Schirmer’s test also tells your eye doctor if your eyes are making enough tears. Your eye doctor will give you eye drops to numb your eye. Then they’ll put a small piece of paper on the edge of your eyelid and ask you to close your eyes for 5 minutes. After 5 minutes, your doctor will see how much moisture (wetness) is on the paper.
Tear break up time (TBUT)
A TBUT test checks how long your tear film (layer of tears on your eyes) lasts after you blink.
Your eye doctor will place a small amount of dye in your eye, and you’ll blink to make the dye fully cover your eye. Then, you’ll look forward without moving your eyes or blinking. Your eye doctor will watch to see how long the dyed tear film covers your whole eye. If your tear film does not last long, you may have dry eye.
Questions:
1. What methods would you use to examine this patient’s tear film quantity?
- A. Phenol red thread test
- B. Schirmer test
- C. Measuring tear meniscus
- D. Any of these methods
2. The tear film meniscus height is measured at 0.05mm using the eye-piece graticule. What grade would you record?
- A. Low
- B. Medium
- C. High
3. What factors could be affecting this patient’s tear quantity?
- A. Age
- B. Environment
- C. Medication
- D. All these factors
4. Which of the following management options could you consider?
- A. Discontinue lens wear
- B. Modify lens fit
- C. Refit with two-weekly replacement silicone hydrogel lenses that are known to perform well in challenging environments
- D. Refit with RGP lenses
Reference:
- visionsource-studio-2020.com
- sciencedirect.com/science/article/abs/pii/S1542012421001518
- uwaterloo.ca/waterloo-eye-institute/news/what-you-should-know-about-dry-eye
- nei.nih.gov/learn-about-eye-health/eye-conditions-and-diseases/dry-eye/testing-dry-eye
- jnjvisionpro.co.uk/education-centre/resource-library/how-assess-and-manage-patients%E2%80%99-tear-film-quantity
 وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.
وبلاگ تخصصی عینک شامل مجموعه مطالب پزشکی است که اطلاعات مفیدی در رابطه با عینک , چشم، لنز، سلامتی چشم و راه های پیشگیری از بیماریهای چشمی، کنترل و درمان آن را در اختیار شما کاربر محترم می گزارد.